

Virologic and immunologic outcomes of treatment with integrase inhibitors in a real-world setting: The RESPOND cohort consortium
- PMID: 33382756
- PMCID: PMC7774984
- DOI: 10.1371/journal.pone.0243625
Virologic and immunologic outcomes of treatment with integrase inhibitors in a real-world setting: The RESPOND cohort consortium
Abstract
Objectives: To compare virologic and immunologic outcomes of integrase inhibitor (INSTI)-containing, contemporary boosted protease inhibitor (PI/b)-containing and non-nucleotide reverse transcriptase inhibitor (NNRTI)-containing regimens in a real-life setting.
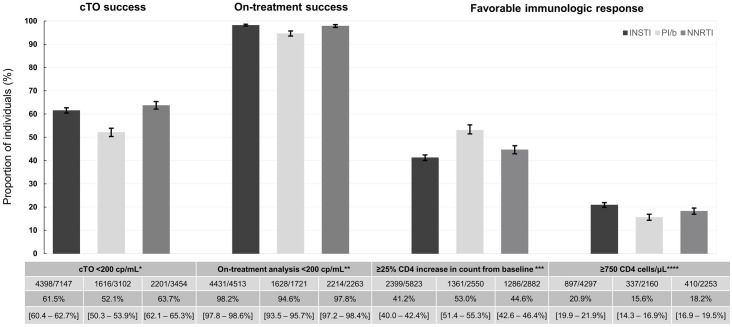
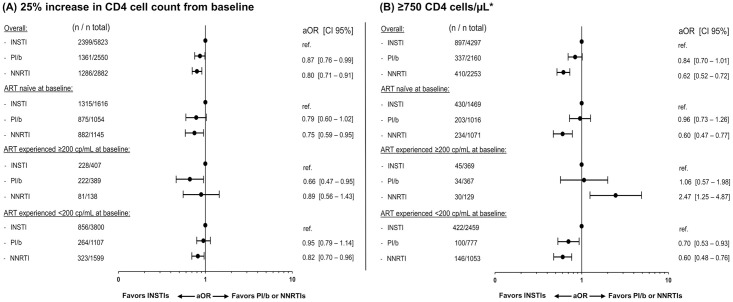
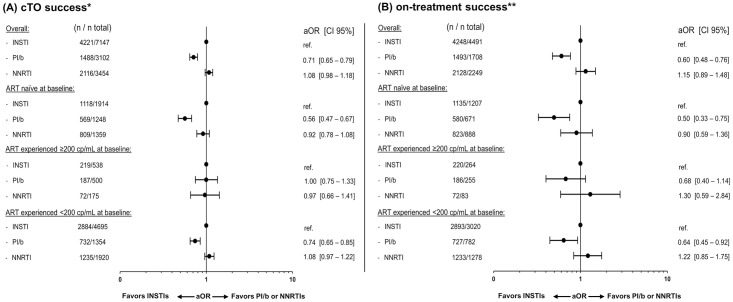
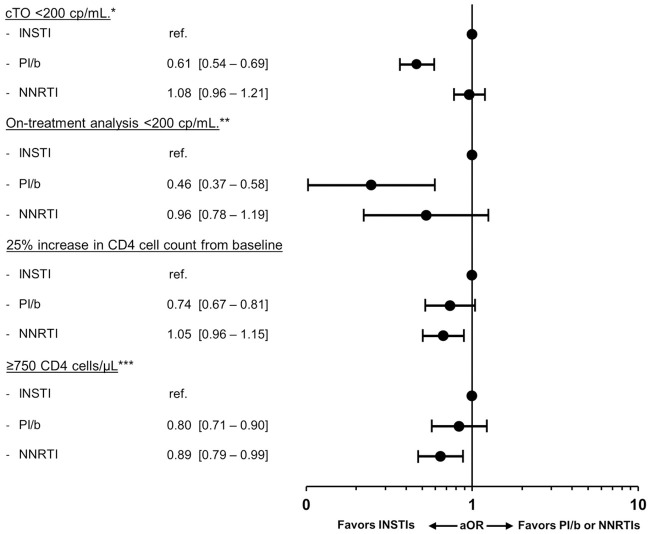
Methods: Using logistic regression, virologic and immunologic outcomes of INSTI use were compared to outcomes of PI/b or NNRTI treatment 12 months after treatment start or switch, for participants in the RESPOND cohort consortium. A composite treatment outcome (cTO) was used, defining success as viral load (VL) <200 copies/mL and failure as at least one of: VL ≥200 copies/mL, unknown VL in the time window, any changes of antiretroviral therapy (ART) regimen, AIDS, or death. In addition, on-treatment analysis including only individuals with known VL and no regimen changes was performed. Favorable immunologic response was defined as a 25% increase in CD4 count or as reaching ≥750 CD4 cells/μL.
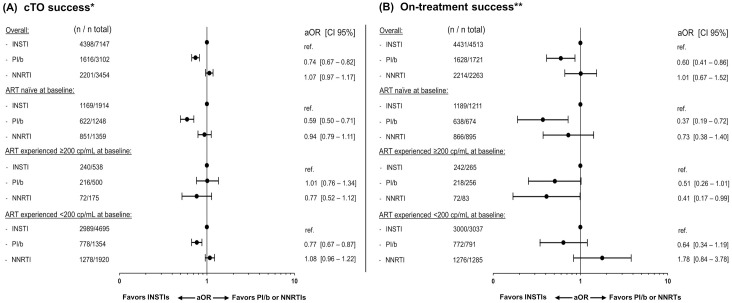
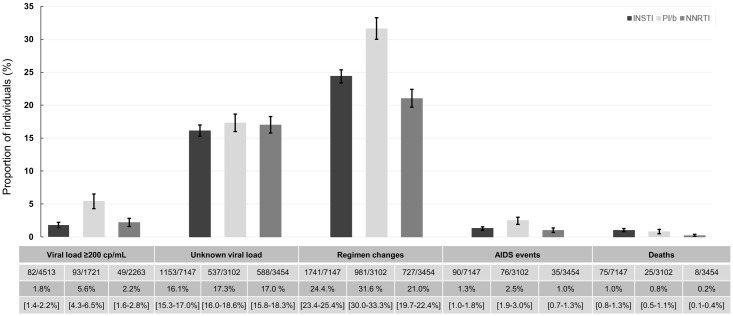
Results: Between January 2012 and January 2019, 13,703 (33.0% ART-naïve) individuals were included, of whom 7,147 started/switched to a regimen with an INSTI, 3,102 to a PI/b and 3,454 to an NNRTI-containing regimen. The main reason for cTO failure in all treatment groups were changes in ART regimen. Compared to INSTIs, the adjusted odds ratio (aOR) of cTO success was significantly lower for PI/b (0.74 [95% confidence interval, CI 0.67-0.82], p <0.001), but similar for NNRTIs (1.07 [CI 0.97-1.17], p = 0.11). On-treatment analysis and sensitivity analyses using a VL cut-off of 50 copies/mL were consistent. Compared to INSTIs, the aORs of a 25% increase in CD4 count were lower for NNRTIs (0.80 [CI 0.71-0.91], p<0.001) and PI/b (0.87 [CI 0.76-0.99], p = 0.04).
Conclusion: In this large analysis of a real-world population, cTO and on-treatment success were similar between INSTIs and NNRTIs, but lower for PI/b, though residual confounding cannot be fully excluded. Obtaining favorable immunologic outcomes were more likely for INSTIs than the other drug classes.
Conflict of interest statement
RESPOND is externally funded by Gilead sciences and ViiV Healthcare. Funding companies have no direct involvement in the conduct of scientific projects. However academic personnel from funders can be included in the writing group for RESPOND projects, if they satisfy the ICMJE criteria, as specified in RESPOND’s governance (https://chip.dk/Portals/0/files/RESPOND/RESPOND%20governance%20and%20procedures_v6_2019SEP30.pdf?ver=2019-10-02-144419-230). This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Clotet B, Feinberg J, van Lunzen J, Khuong-Josses MA, Antinori A, Dumitru I, et al. Once-daily dolutegravir versus darunavir plus ritonavir in antiretroviral-naive adults with HIV-1 infection (FLAMINGO): 48 week results from the randomised open-label phase 3b study. Lancet. 2014;383(9936):2222–31. Epub 2014/04/05. 10.1016/S0140-6736(14)60084-2 . - DOI - PubMed
-
- Molina JM, Clotet B, van Lunzen J, Lazzarin A, Cavassini M, Henry K, et al. Once-daily dolutegravir versus darunavir plus ritonavir for treatment-naive adults with HIV-1 infection (FLAMINGO): 96 week results from a randomised, open-label, phase 3b study. Lancet HIV. 2015;2(4):e127–36. Epub 2015/10/02. 10.1016/S2352-3018(15)00027-2 . - DOI - PubMed
-
- Molina JM, Lamarca A, Andrade-Villanueva J, Clotet B, Clumeck N, Liu YP, et al. Efficacy and safety of once daily elvitegravir versus twice daily raltegravir in treatment-experienced patients with HIV-1 receiving a ritonavir-boosted protease inhibitor: randomised, double-blind, phase 3, non-inferiority study. Lancet Infect Dis. 2012;12(1):27–35. Epub 2011/10/22. 10.1016/S1473-3099(11)70249-3 . - DOI - PubMed
-
- Sax PE, DeJesus E, Mills A, Zolopa A, Cohen C, Wohl D, et al. Co-formulated elvitegravir, cobicistat, emtricitabine, and tenofovir versus co-formulated efavirenz, emtricitabine, and tenofovir for initial treatment of HIV-1 infection: a randomised, double-blind, phase 3 trial, analysis of results after 48 weeks. Lancet. 2012;379(9835):2439–48. Epub 2012/07/04. 10.1016/S0140-6736(12)60917-9 . - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
