

The role of CPAP as a potential bridge to invasive ventilation and as a ceiling-of-care for patients hospitalized with Covid-19-An observational study
- PMID: 33382796
- PMCID: PMC7774971
- DOI: 10.1371/journal.pone.0244857
The role of CPAP as a potential bridge to invasive ventilation and as a ceiling-of-care for patients hospitalized with Covid-19-An observational study
Abstract
Background: Continuous positive airway pressure (CPAP) ventilation may be used as a potential bridge to invasive mechanical ventilation (IMV), or as a ceiling-of-care for persistent hypoxaemia despite standard oxygen therapy, according to UK guidelines. We examined the association of mode of respiratory support and ceiling-of-care on mortality.
Methods: We conducted a retrospective cohort analysis of routinely collected de-identified data of adults with nasal/throat SARs-CoV-2 swab-positive results, at the Calderdale and Huddersfield NHS Foundation Trust between 10th March-19th April 2020 (outcomes determined on 22nd May).
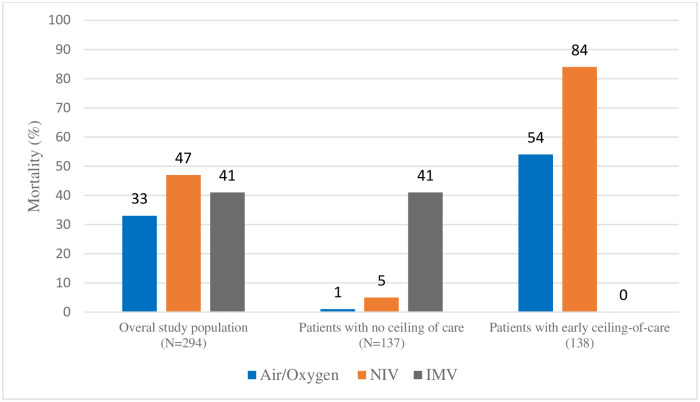
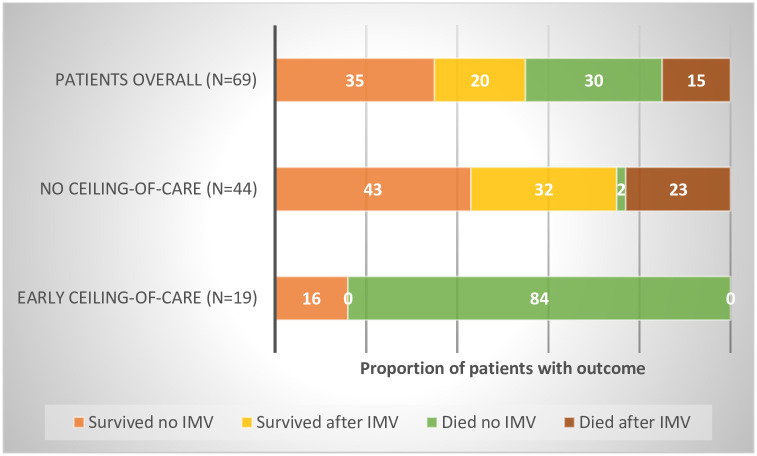
Findings: Of 347 patients with SARs-CoV-2 swab-positive results, 294 (84.7%) patients admitted for Covid-19 were included in the study. Sixty-nine patients were trialled on CPAP, mostly delivered by face mask, either as an early ceiling of care instituted within 24 hours of admission (N = 19), or as a potential bridge to IMV (N = 44). Patients receiving a ceiling of care more than 24 hours after admission (N = 6) were excluded from the analysis. Two hundred and fifteen patients (73.1%) maximally received air/standard oxygen therapy, and 45 (15.3%) patients maximally received CPAP. Thirty-four patients (11.6%) required IMV, of which 24 had received prior CPAP. There were 138 patients with an early ceiling-of-care plan (pre-admission/within 24h). Overall, 103(35.0%) patients died and 191(65.0%) were alive at study end. Among all patients trialled on CPAP either as a potential bridge to IMV (N = 44) or as a ceiling-of-care (N = 19) mortality was 25% and 84%, respectively. Overall, there was strong evidence for higher mortality among patients who required CPAP or IMV, compared to those who required only air/oxygen (aOR 5.24 95%CI: 1.38, 19.81 and aOR 46.47 95%CI: 7.52, 287.08, respectively; p<0.001), and among patients with early ceiling-of-care compared to those without a ceiling (aOR 41.81 95%CI: 8.28, 211.17; p<0.001). Among patients without a ceiling of care (N = 137), 10 patients required prompt intubation following failed oxygen therapy, but 44 patients received CPAP. CPAP failure, defined as death (N = 1) or intubation (N = 24), occurred in 57% (N = 25) of patients. But in total, 75% (N = 33) of those started on CPAP with no ceiling of care recovered to discharge-19 without the need for IMV, and 14 following IMV.
Conclusion: Our data suggest that among patients with no ceiling-of-care, an initial trial of CPAP as a potential bridge to IMV offers a favourable therapeutic alternative to early intubation. In contrast, among patients with a ceiling-of care, CPAP seems to offer little additional survival benefit beyond oxygen therapy alone. Information on ceilings of respiratory support is vital to interpreting mortality from Covid-19.
Strengths and limitations of this study: Sample size relatively small.Study sample representative of hospitalised Covid-19 patients in UK.Previously unreported data on role of ceilings-of-care in hospitalised Covid-19 patients.Novel data on use of CPAP separated by indication.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Johns Hopkins University. Coronavirus Resource Centre Maps and Trends. https://coronavirus.jhu.edu/maphtml. 2020:Accessed on 11th June 2020.
-
- Intensive Care National Research and Audit Centre. ICNARC Report on Covid-19 in Critical Care (12th June 2020). https://www.icnarc.org/Our-Audit/Audits/Cmp/Reports. 2020:Accessed 16th June 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
