

Visceral Adiposity, Pro-Inflammatory Signaling and Vasculopathy in Metabolically Unhealthy Non-Obesity Phenotype
- PMID: 33383705
- PMCID: PMC7824214
- DOI: 10.3390/diagnostics11010040
Visceral Adiposity, Pro-Inflammatory Signaling and Vasculopathy in Metabolically Unhealthy Non-Obesity Phenotype
Abstract
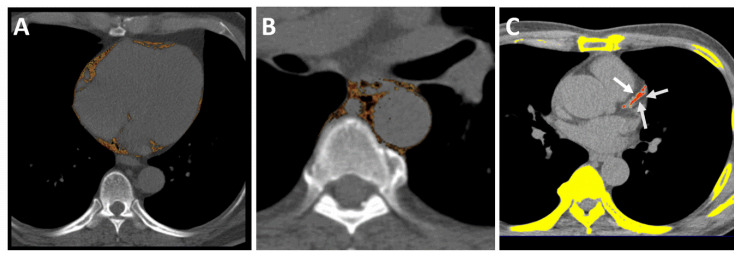
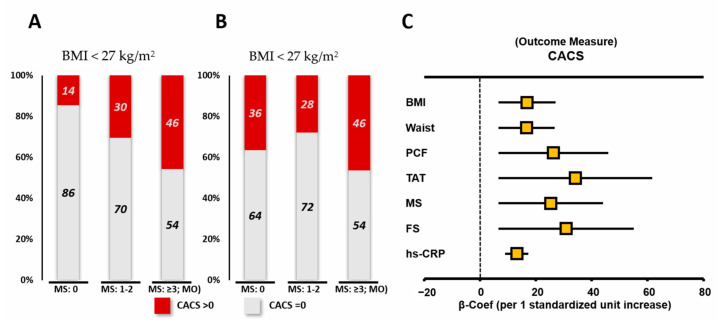
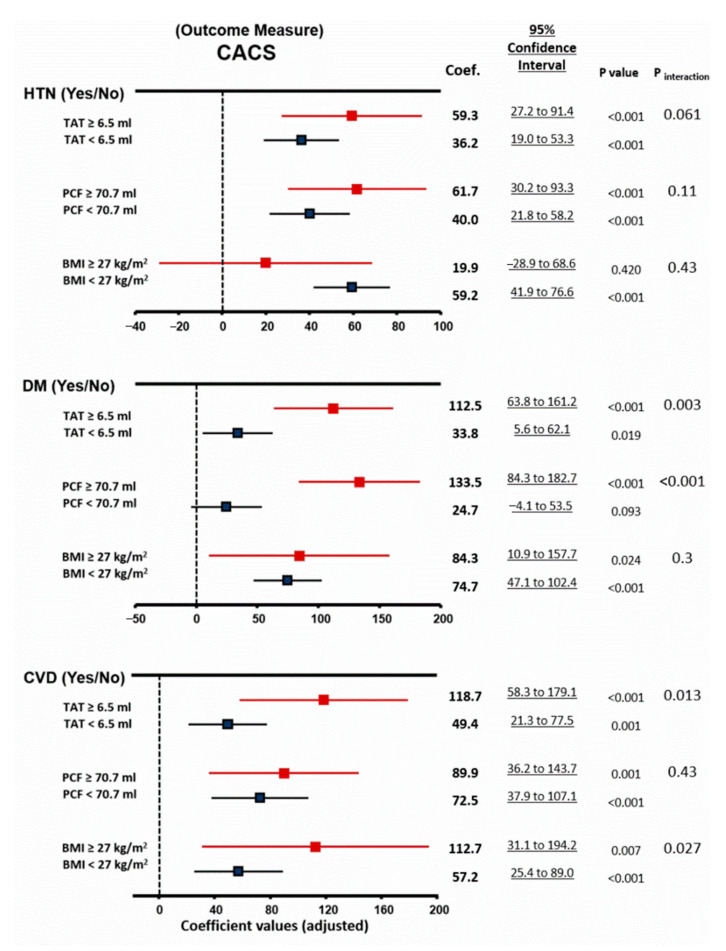
The debate regarding the actual cardiovascular burden in metabolically healthy obese or metabolically unhealthy non-obesity individuals is ongoing. Accumulating data have suggested a unique pathophysiological role of pro-inflammatory cytokines in mediating metabolic and cardiovascular disorders by dysregulated visceral adiposity. To compare the burden of visceral adiposity, the inflammatory marker high-sensitivity C-reactive protein (hs-CRP) and the prevalent atherosclerotic burden in metabolically healthy obese (MHO) or metabolically unhealthy (MU) populations, were compared to those of metabolically healthy non-obesity subjects (MHNO). Coronary artery calcification score (CACS) and visceral fat, including pericardial fat (PCF)/thoracic peri-aortic fat (TAT), were quantified in 2846 asymptomatic subjects using a CT dataset. A cross-sectional analysis comparing CACS, inflammatory marker hs-CRP, and visceral fat burden among four obesity phenotypes (MHNO, metabolically unhealthy non-obesity (MUNO), MHO, and metabolically unhealthy obese (MUO)) was performed. Both MUNO and MUO demonstrated significantly higher hs-CRP and greater CACS than MHNO/MHO (adjusted coefficient: 25.46, 95% confidence interval (CI): 5.29-45.63; 43.55, 95% CI: 23.38-63.73 for MUNO and MUO (MHNO as reference); both p < 0.05). Visceral fat (PCF/TAT) was an independent determinant of MU and was similarly higher in the MUNO/MHO groups than in the MHNO group, with the MUO group having the largest amount. PCF/TAT, obesity, and MU remained significantly associated with higher CACS even after adjustment, with larger PCF/TAT modified effects for MU and diabetes in CACS (both pinteraction < 0.05). MU tightly linked to excessive visceral adiposity was a strong and independent risk factor for coronary atherosclerosis even in lean individuals, which could be partially explained by its coalignment with pathological pro-inflammatory signaling.
Keywords: coronary artery calcification score (CACS); hs-CRP; metabolically unhealthy; obese phenotype; visceral adiposity.
Conflict of interest statement
The authors have no conflict of interest.
Figures
Similar articles
-
Differences in the levels of inflammatory markers between metabolically healthy obese and other obesity phenotypes in adults: A systematic review and meta-analysis.Nutr Metab Cardiovasc Dis. 2024 Feb;34(2):251-269. doi: 10.1016/j.numecd.2023.09.002. Epub 2023 Sep 9. Nutr Metab Cardiovasc Dis. 2024. PMID: 37968171
-
Echocardiographic Assessment in Various Obesity Phenotypes: A Cross-Sectional Study.Cureus. 2025 Feb 7;17(2):e78716. doi: 10.7759/cureus.78716. eCollection 2025 Feb. Cureus. 2025. PMID: 40065855 Free PMC article.
-
The Association between Cardio-metabolic and hepatic indices and anthropometric measures with metabolically obesity phenotypes: a cross-sectional study from the Hoveyzeh Cohort Study.BMC Endocr Disord. 2023 May 29;23(1):122. doi: 10.1186/s12902-023-01372-9. BMC Endocr Disord. 2023. PMID: 37246210 Free PMC article.
-
Association between obese phenotypes and risk of carotid artery plaque among chinese male railway drivers.BMC Public Health. 2022 Oct 5;22(1):1859. doi: 10.1186/s12889-022-14253-y. BMC Public Health. 2022. PMID: 36199053 Free PMC article.
-
Epidemiology and pathophysiology of the association between NAFLD and metabolically healthy or metabolically unhealthy obesity.Ann Hepatol. 2020 Jul-Aug;19(4):359-366. doi: 10.1016/j.aohep.2020.03.001. Epub 2020 Mar 21. Ann Hepatol. 2020. PMID: 32349939 Review.
Cited by
-
Relationship Between Zinc, Selenium, and Magnesium Status and Markers of Metabolically Healthy and Unhealthy Obesity Phenotypes.Biol Trace Elem Res. 2024 Aug;202(8):3449-3464. doi: 10.1007/s12011-023-03938-z. Epub 2023 Nov 14. Biol Trace Elem Res. 2024. PMID: 37957519
-
Triglyceride glucose-weight-adjusted waist index (TyG-WWI): the best predictor of diabetes mellitus and mortality risks among TyG and TyG-derived indices.BMC Endocr Disord. 2025 Jul 4;25(1):166. doi: 10.1186/s12902-025-01989-y. BMC Endocr Disord. 2025. PMID: 40616082 Free PMC article.
-
Platelet-rich plasma does not improve clinical results in patients with rotator cuff disorders but reduces the retear rate. A systematic review and meta-analysis.Knee Surg Sports Traumatol Arthrosc. 2023 May;31(5):1940-1952. doi: 10.1007/s00167-022-07223-9. Epub 2022 Dec 11. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36496450
-
Obesity and Endothelial Function.Biomedicines. 2022 Jul 19;10(7):1745. doi: 10.3390/biomedicines10071745. Biomedicines. 2022. PMID: 35885049 Free PMC article. Review.
-
PM2.5, component cause of severe metabolically abnormal obesity: An in silico, observational and analytical study.Heliyon. 2024 Apr 3;10(7):e28936. doi: 10.1016/j.heliyon.2024.e28936. eCollection 2024 Apr 15. Heliyon. 2024. PMID: 38601536 Free PMC article.
References
-
- Kuwabara M., Kuwabara R., Hisatome I., Niwa K., Roncal-Jimenez C.A., Bjornstad P., Andres-Hernando A., Sato Y., Jensen T., Garcia G., et al. Metabolically Healthy Obesity and Hyperuricemia Increase Risk for Hypertension and Diabetes: 5-year Japanese Cohort Study. Obesity. 2017;25:1997–2008. doi: 10.1002/oby.22000. - DOI - PMC - PubMed
-
- Kwon B.-J., Kim D.-W., Her S.-H., Kim D.-B., Jang S.-W., Cho E.-J., Ihm S.H., Kim H.-Y., Youn H.-J., Seung K.-B., et al. Metabolically obese status with normal weight is associated with both the prevalence and severity of angiographic coronary artery disease. Metabolism. 2013;62:952–960. doi: 10.1016/j.metabol.2013.01.006. - DOI - PubMed
-
- Kip K.E., Marroquin O.C., Kelley D.E., Johnson B.D., Kelsey S.F., Shaw L.J., Rogers W.J., Reis S.E. Clinical importance of obesity versus the metabolic syndrome in cardiovascular risk in women: A report from the Women’s Ischemia Syndrome Evaluation (WISE) study. Circulation. 2004;109:706–713. doi: 10.1161/01.CIR.0000115514.44135.A8. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
