

End-of-Life Care Preferences of Older Patients with Multimorbidity: A Mixed Methods Systematic Review
- PMID: 33383951
- PMCID: PMC7795676
- DOI: 10.3390/jcm10010091
End-of-Life Care Preferences of Older Patients with Multimorbidity: A Mixed Methods Systematic Review
Abstract
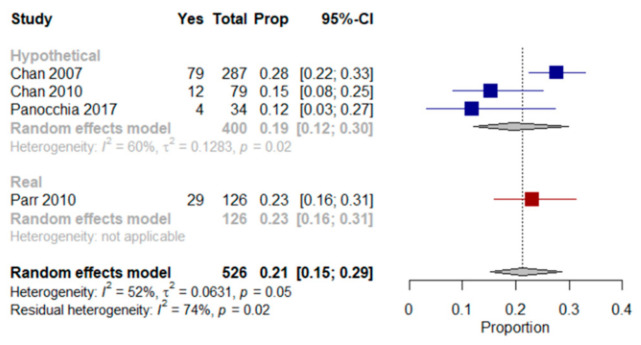
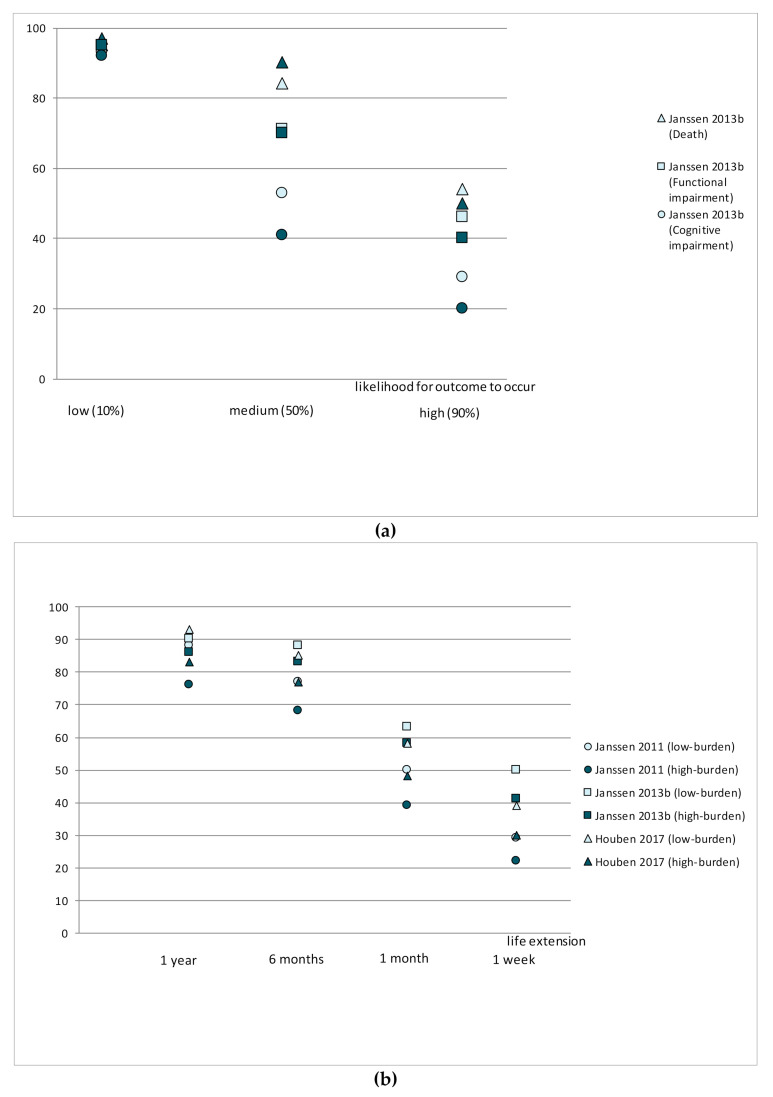
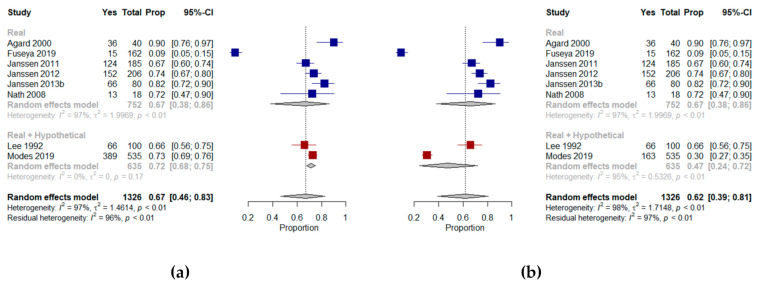
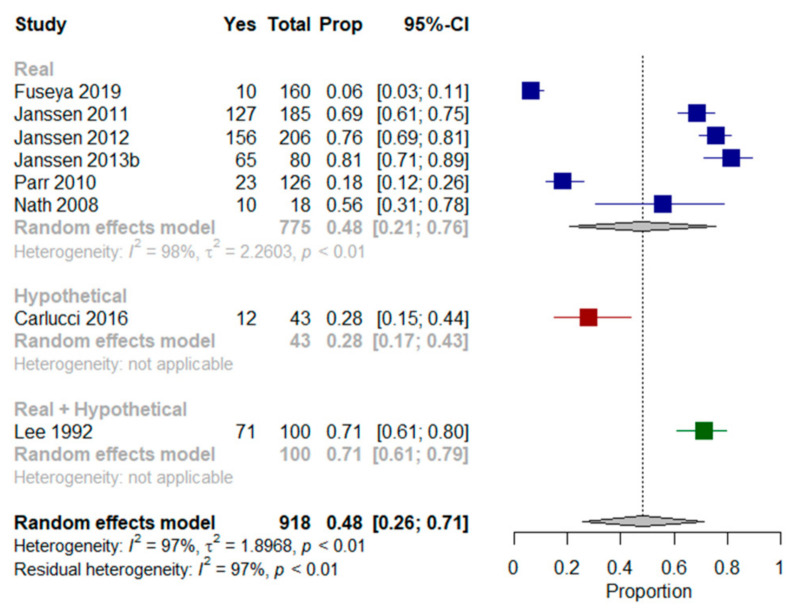
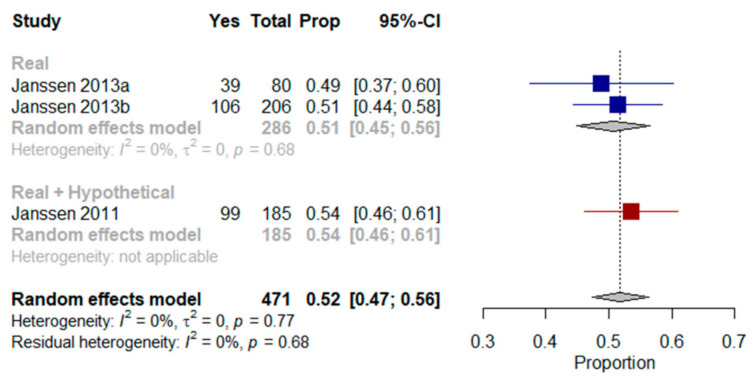
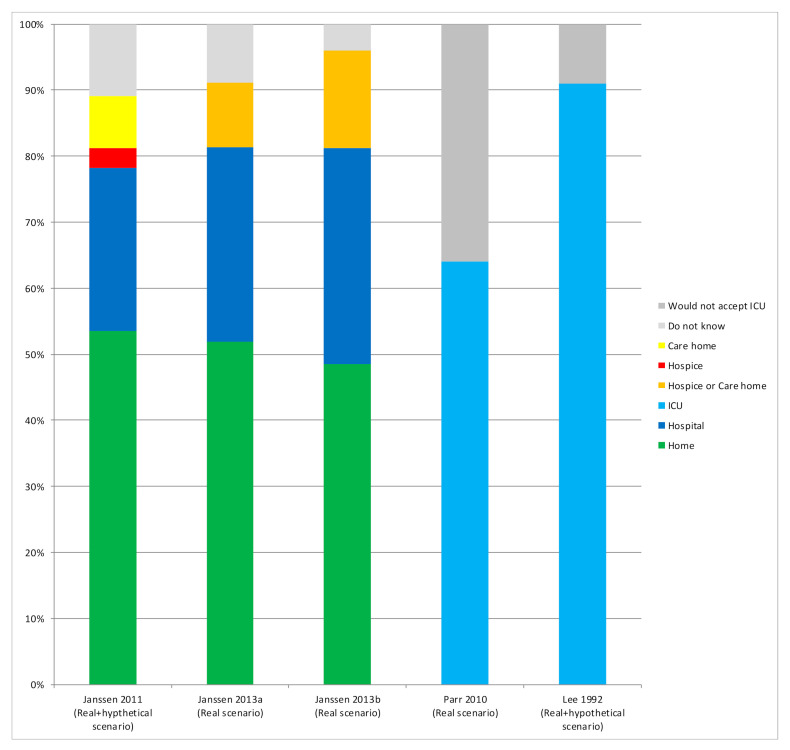
Unpredictable disease trajectories make early clarification of end-of-life (EoL) care preferences in older patients with multimorbidity advisable. This mixed methods systematic review synthesizes studies and assesses such preferences. Two independent reviewers screened title/abstracts/full texts in seven databases, extracted data and used the Mixed Methods Appraisal Tool to assess risk of bias (RoB). We synthesized findings from 22 studies (3243 patients) narratively and, where possible, quantitatively. Nineteen studies assessed willingness to receive life-sustaining treatments (LSTs), six, the preferred place of care, and eight, preferences regarding shared decision-making processes. When unspecified, 21% of patients in four studies preferred any LST option. In three studies, fewer patients chose LST when faced with death and deteriorating health, and more when treatment promised life extension. In 13 studies, 67% and 48% of patients respectively were willing to receive cardiopulmonary resuscitation and mechanical ventilation, but willingness decreased with deteriorating health. Further, 52% of patients from three studies wished to die at home. Seven studies showed that unless incapacitated, most patients prefer to decide on their EoL care themselves. High non-response rates meant RoB was high in most studies. Knowledge of EoL care preferences of older patients with multimorbidity increases the chance such care will be provided.
Keywords: elderly; end of life care; multimorbidity; patient centered care; patient preferences.
Conflict of interest statement
The authors declare no conflict of interest. The funder had no role in the design of the study, in the collection, analyses or interpretation of data, in writing the manuscript, or in the decision to publish the results.
Figures
References
-
- National Institute for Health Care Excellence End of Life Care for Adults: Service Delivery (NG142) [(accessed on 19 June 2020)]; Available online: https://www.nice.org.uk/guidance/ng142.
-
- Lynn J., Teno J.M., Phillips R.S., Wu A.W., Desbiens N., Harrold J., Claessens M.T., Wenger N., Kreling B., Connors A.F., Jr. Perceptions by family members of the dying experience of older and seriously ill patients. SUPPORT Investigators. Study to understand prognoses and preferences for outcomes and risks of treatments. Ann. Intern. Med. 1997;126:97–106. doi: 10.7326/0003-4819-126-2-199701150-00001. - DOI - PubMed
-
- Lynn J. Living Long in Fragile Health. The New Demographics Shape End of Life Care. [(accessed on 29 June 2020)]; Available online: https://www.rand.org/pubs/reprints/RP1200.html. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
