

Clinical Outcomes in Patients With Heart Failure Hospitalized With COVID-19
- PMID: 33384064
- PMCID: PMC7833294
- DOI: 10.1016/j.jchf.2020.11.003
Clinical Outcomes in Patients With Heart Failure Hospitalized With COVID-19
Abstract
Objectives: The purpose of this study was to evaluate in-hospital outcomes among patients with a history of heart failure (HF) hospitalized with coronavirus disease-2019 (COVID-19).
Background: Cardiometabolic comorbidities are common in patients with severe COVID-19. Patients with HF may be particularly susceptible to COVID-19 complications.
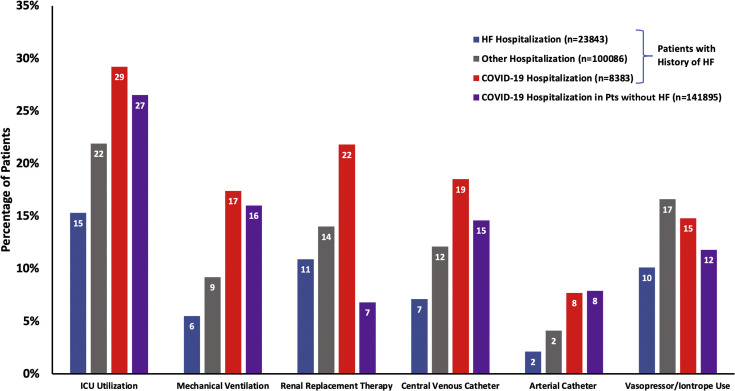
Methods: The Premier Healthcare Database was used to identify patients with at least 1 HF hospitalization or 2 HF outpatient visits between January 1, 2019, and March 31, 2020, who were subsequently hospitalized between April and September 2020. Baseline characteristics, health care resource utilization, and mortality rates were compared between those hospitalized with COVID-19 and those hospitalized with other causes. Predictors of in-hospital mortality were identified in HF patients hospitalized with COVID-19 by using multivariate logistic regression.
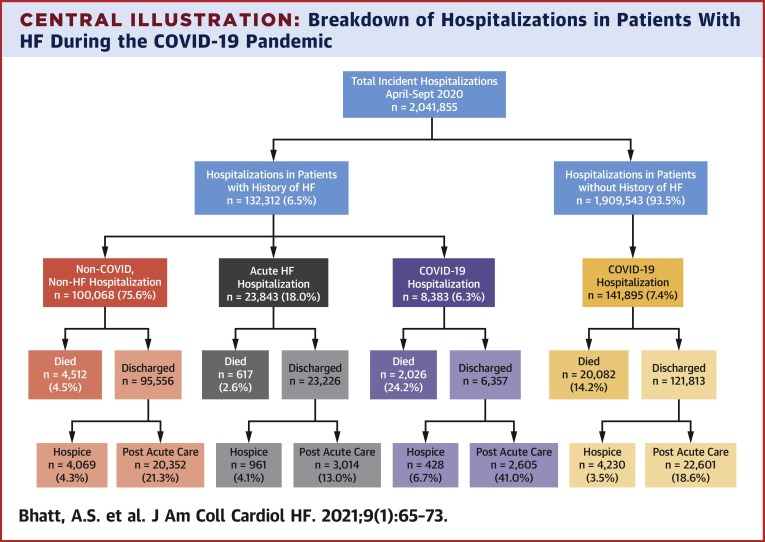
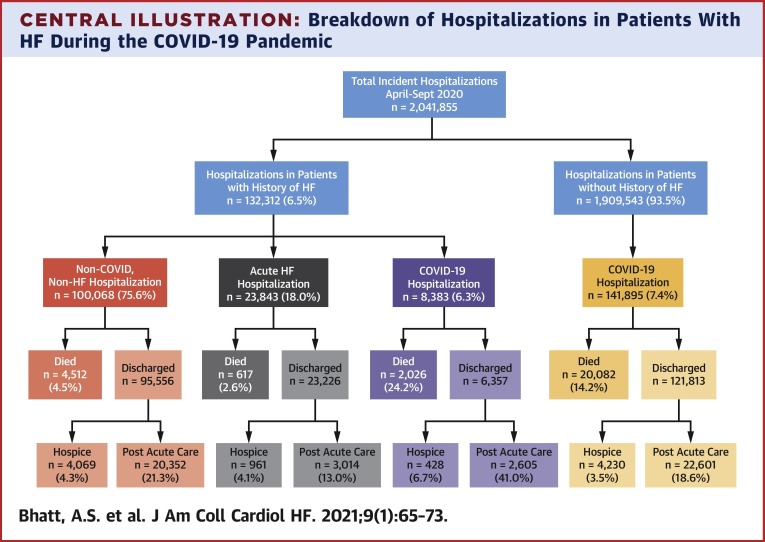
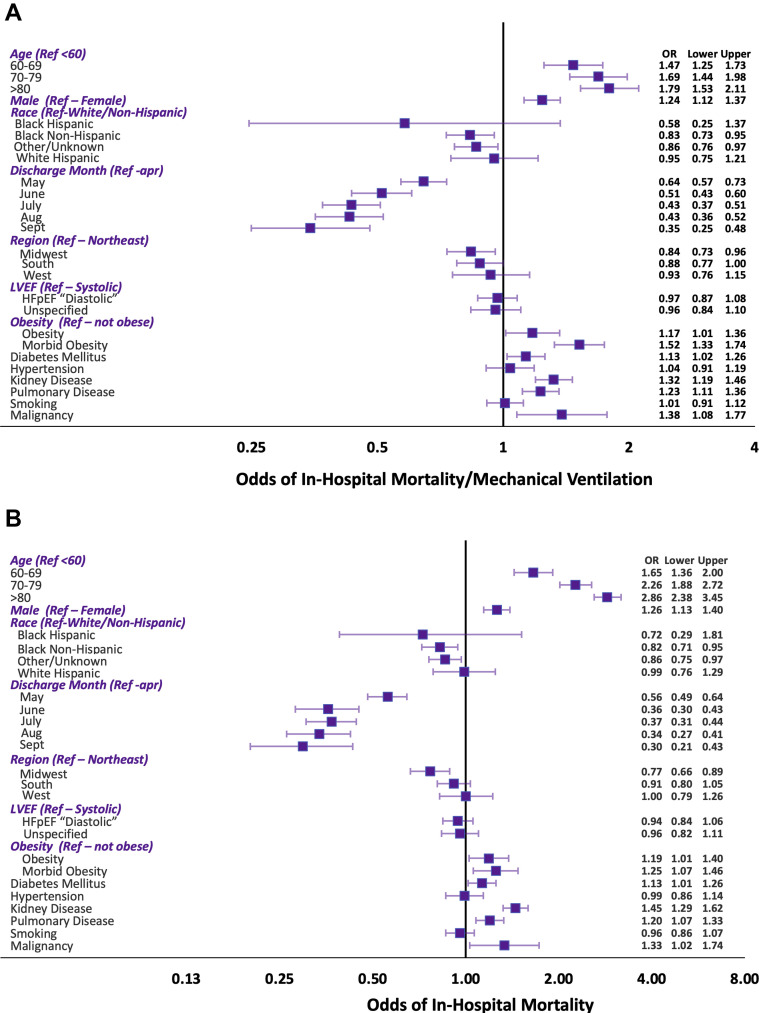
Results: Among 1,212,153 patients with history of HF, 132,312 patients were hospitalized from April 1, 2020, to September 30, 2020. A total of 23,843 patients (18.0%) were hospitalized with acute HF, 8,383 patients (6.4%) were hospitalized with COVID-19, and 100,068 patients (75.6%) were hospitalized with alternative reasons. Hospitalization with COVID-19 was associated with greater odds of in-hospital mortality as compared with hospitalization with acute HF; 24.2% of patients hospitalized with COVID-19 died in-hospital compared to 2.6% of those hospitalized with acute HF. This association was strongest in April (adjusted odds ratio [OR]: 14.48; 95% confidence interval [CI]:12.25 to 17.12) than in subsequent months (adjusted OR: 10.11; 95% CI: 8.95 to 11.42; pinteraction <0.001). Among patients with HF hospitalized with COVID-19, male sex (adjusted OR: 1.26; 95% CI: 1.13 to 1.40) and morbid obesity (adjusted OR: 1.25; 95% CI: 1.07 to 1.46) were associated with greater odds of in-hospital mortality, along with age (adjusted OR: 1.35; 95% CI: 1.29 to 1.42 per 10 years) and admission earlier in the pandemic.
Conclusions: Patients with HF hospitalized with COVID-19 are at high risk for complications, with nearly 1 in 4 dying during hospitalization.
Keywords: COVID-19; coronavirus; heart failure.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author Disclosures Dr. Bhatt has received speaker fees from Sanofi Pasteur; and is supported by National Heart, Lung, and Blood Institute T32 post-doctoral training grant T32HL007604. Dr. Jering is supported by National Heart, Lung, and Blood Institute T32 post-doctoral training grant T32HL007604. Dr. Vaduganathan has received grants from Harvard Catalyst, grants and personal fees from Amgen, and personal fees from AstraZeneca, Baxter HealthCare, Bayer AG, Boehringer Ingelheim, Cytokinetics, and Relypsa outside the submitted work. Dr. Claggett has received personal fees from Amgen, Boehringer Ingelheim, Corvia, MyoKardia, and Novartis outside the submitted work. Dr. Cunningham is supported by National Heart, Lung, and Blood Institute T32 post-doctoral training grant T32HL007604. Dr. Rosenthal is an employee of Premier Inc., which curates the Premier Healthcare Database. Dr. Signorovitch is an employee of Analysis Group, Inc. Dr. Thune has received lecture fees from Bristol-Myers Squibb; and has received personal fees and travel support from Novartis. Dr. Vardeny has received research support from U.S. National Institutes of Health; and is a consultant for Sanofi-Pasteur. Dr. Solomon has received grants from Alnylam, Amgen, AstraZeneca, Bellerophon, Bayer, Bristol-Myers Squibb, Celladon, Cytokinetics, Eidos, Gilead, GlaxoSmithKline, Ionis, Lone Star Heart, Mesoblast, MyoKardia, Neurotronik, National Institutes of Health/National Heart, Lung, and Blood Institute, Novartis, Respicardia, Sanofi Pasteur, and Theracos; and has received personal fees from Akros, Alnylam, Amgen, Arena, AstraZeneca, Bayer, Bristol-Meyers Squibb, Cardior, Cardurion, Corvia, Cytokinetics, Daiichi-Sankyo, Gilead, GlaxoSmithKline, Ironwood, Merck, Myokardia, Novartis, Roche, Takeda, Theracos, Quantum Genetics, Cardurion, AoBiome, Janssen, Cardiac Dimensions, Sanofi-Pasteur, Tenaya, Dinaqor, Tremeau, CellProThera, and Moderna outside the submitted work.
Figures
Comment in
-
Promoting Health Equity in Heart Failure Amid a Pandemic.JACC Heart Fail. 2021 Jan;9(1):74-76. doi: 10.1016/j.jchf.2020.11.002. JACC Heart Fail. 2021. PMID: 33384065 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
