

Periprocedural complications in patients with SARS-CoV-2 infection compared to those without infection: A nationwide propensity-matched analysis
- PMID: 33384154
- PMCID: PMC7836786
- DOI: 10.1016/j.amjsurg.2020.12.024
Periprocedural complications in patients with SARS-CoV-2 infection compared to those without infection: A nationwide propensity-matched analysis
Abstract
Background: Reports on emergency surgery performed soon after a COVID-19 infection that are not controlled for premorbid risk-factors show increased 30-day mortality and pulmonary complications. This contributed to a virtual cessation of elective surgery during the pandemic surge. To inform evidence-based guidance on the decisions for surgery during the recovery phase of the pandemic, we compare 30-day outcomes in patients testing positive for COVID-19 before their operation, to contemporary propensity-matched COVID-19 negative patients undergoing the same procedures.
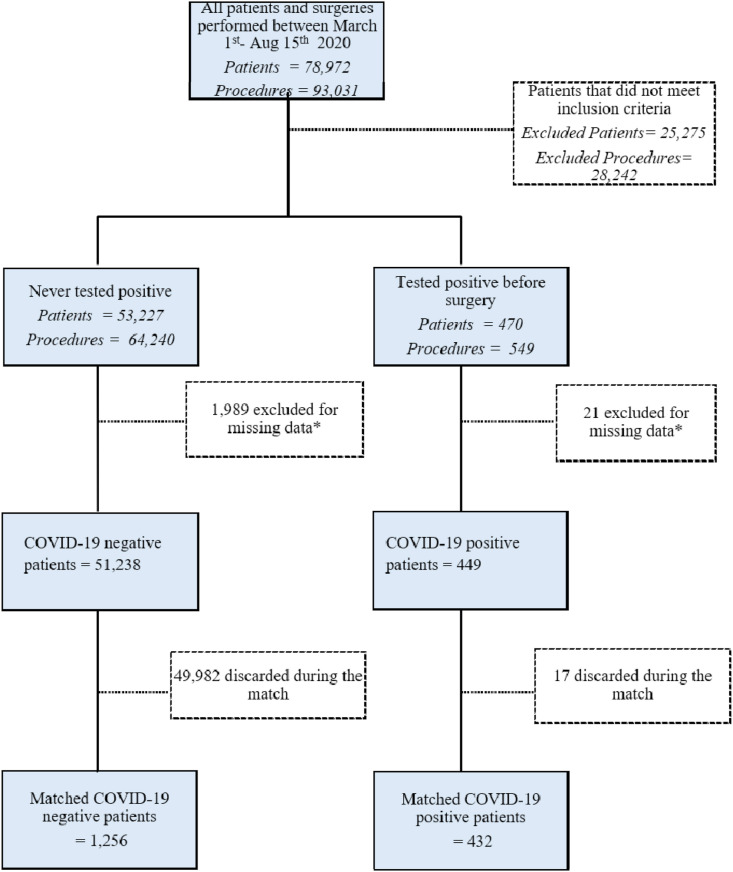
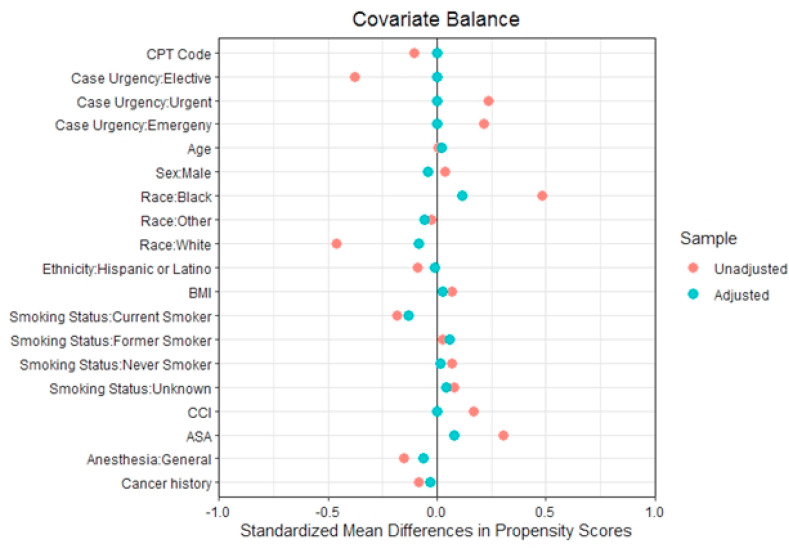
Methods: This prospective multicentre study included all patients undergoing surgery at 170 Veterans Health Administration (VA) hospitals across the United States. COVID-19 positive patients were propensity matched to COVID-19 negative patients on demographic and procedural factors. We compared 30-day outcomes between COVID-19 positive and negative patients, and the effect of time from testing positive to the date of procedure (≤10 days, 11-30 days and >30 days) on outcomes.
Results: Between March 1 and August 15, 2020, 449 COVID-19 positive and 51,238 negative patients met inclusion criteria. Propensity matching yielded 432 COVID-19 positive and 1256 negative patients among whom half underwent elective surgery. Infected patients had longer hospital stays (median seven days), higher rates of pneumonia (20.6%), ventilator requirement (7.6%), acute respiratory distress syndrome (ARDS, 17.1%), septic shock (13.7%), and ischemic stroke (5.8%), while mortality, reoperations and readmissions were not significantly different. Higher odds for ventilation and stroke persisted even when surgery was delayed 11-30 days, and for pneumonia, ARDS, and septic shock >30 days after a positive test.
Discussion: 30-day pulmonary, septic, and ischaemic complications are increased in COVID-19 positive, compared to propensity score matched negative patients. Odds for several complications persist despite a delay beyond ten days after testing positive. Individualized risk-stratification by pulmonary and atherosclerotic comorbidities should be considered when making decisions for delaying surgery in infected patients.
Keywords: Adult; COVID-19; Operative; Postoperative complications; Respiratory distress syndrome; Risk factors; Surgical procedures.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest We declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
