

Impact of Bedside Combined Cardiopulmonary Ultrasound on Etiological Diagnosis and Treatment of Acute Respiratory Failure in Critically Ill Patients
- PMID: 33384512
- PMCID: PMC7751041
- DOI: 10.5005/jp-journals-10071-23661
Impact of Bedside Combined Cardiopulmonary Ultrasound on Etiological Diagnosis and Treatment of Acute Respiratory Failure in Critically Ill Patients
Abstract
Aims and objectives: To prospectively evaluate the impact of cardiopulmonary ultrasound (CPUS) on etiological diagnosis and treatment of critically ill acute respiratory failure (ARF) patients.
Design: This is a prospective observational study conducted in a general intensive care unit (ICU) of a tertiary care center in India. Patients over 18 years old with presence of one of the objective criteria of ARF. Patients either consecutively admitted for ARF to ICU or already admitted to ICU for a different reason but later developed ARF during their hospital stay. Written informed consent in local language was obtained from next of kin.
Interventions: All included patients underwent bedside CPUS including lung ultrasound (US) and transthoracic echocardiography plus targeted venous US by single investigator, blinded to clinical data. The US diagnosis of ARF etiology was shared with treating intensivist. Initial clinical diagnosis (ICD) and treatment plan (made before US) of each patient were compared with post-US clinical diagnosis and treatment plan. The changes in diagnosis and treatment up to 24 hours post-US were considered as impact of US.
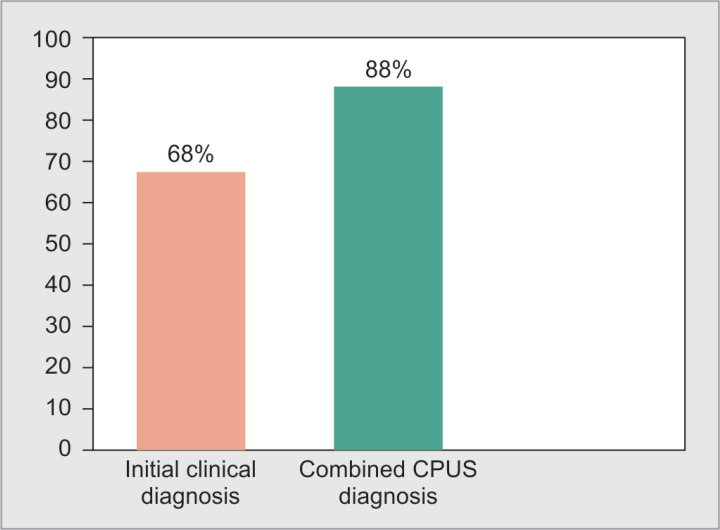
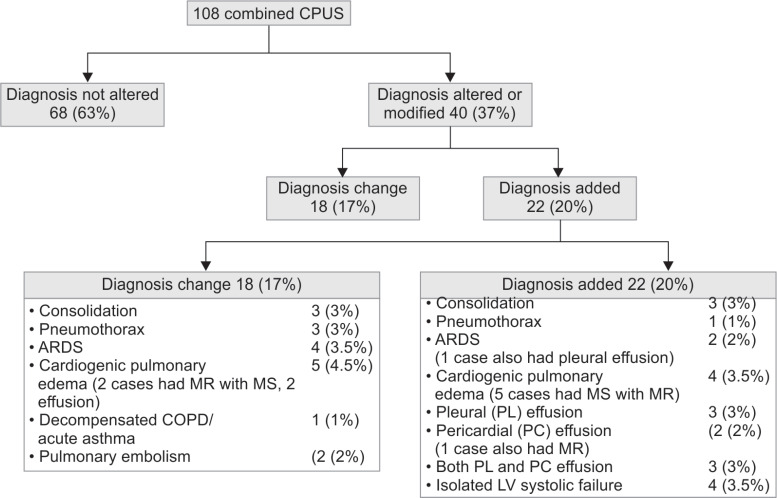
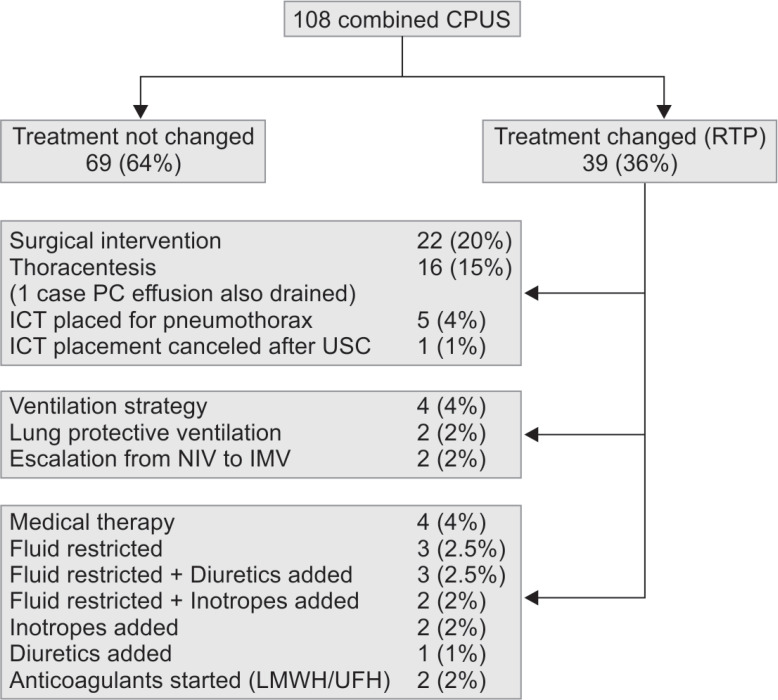
Results: Mean age of 108 included patients was 45.7 ± 20.4 years (standard deviation). The ICD was correct in 67.5% (73/108) cases, whereas the combined CPUS yielded correct etiological diagnosis in 88% (95/108) cases. Among the 108 included patients, etiological diagnosis of ARF was altered after CPUS in 40 (37%) patients, which included "diagnosis changed" in 18 (17%) and "diagnosis added" in 22 (20%). Treatment plan was changed in 39 (36%) patients after CPUS, which included surgical interventions in 17 (16%), changes in medical therapy in 12 (11%), and changes in ventilation strategy in 4 (3.5%) patients.
Conclusion: This study demonstrates that use of combined US approach as an initial test in ARF, improves diagnostic accuracy for identification of underlying etiology, and frequently changes clinical diagnosis and/or treatment.
How to cite this article: Barman B, Parihar A, Kohli N, Agarwal A, Dwivedi DK, Kumari G. Impact of Bedside Combined Cardiopulmonary Ultrasound on Etiological Diagnosis and Treatment of Acute Respiratory Failure in Critically Ill Patients. Indian J Crit Care Med 2020;24(11):1062-1070.
Keywords: Acute respiratory failure; Combined ultrasound approach; Critical care; Impact assessment; Lung ultrasound; Transthoracic echocardiography.
Copyright © 2020; Jaypee Brothers Medical Publishers (P) Ltd.
Conflict of interest statement
Source of support: Nil Conflict of interest: None
Figures
References
-
- International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10). Respiratory failure, 2018. https://www.icd10data.com/ICD10CM/Codes/J00-J99/J96-J99/J96-/J96.0 https://www.icd10data.com/ICD10CM/Codes/J00-J99/J96-J99/J96-/J96.0 - PubMed
-
- Neto AS, Barbas CSV, Simonis FD, Artigas-Raventós A, Canet J, Determann RM, et al. Epidemiological characteristics, practice of ventilation, and clinical outcome in patients at risk of acute respiratory distress syndrome in intensive care units from 16 countries (PRoVENT): an international, multicentre, prospective study. Lancet Respir Med. 2016;4(11):882–893. doi: 10.1016/S2213-2600(16)30305-8. DOI: - DOI - PubMed
LinkOut - more resources
Full Text Sources