

Prevalence and associated factors of obesity in inflammatory bowel disease: A case-control study
- PMID: 33384552
- PMCID: PMC7754553
- DOI: 10.3748/wjg.v26.i47.7528
Prevalence and associated factors of obesity in inflammatory bowel disease: A case-control study
Abstract
Background: In recent years, an increasing prevalence of obesity in inflammatory bowel disease (IBD) has been observed. Obesity, moreover, has been directly correlated with a more severe clinical course and loss of response to treatment.
Aim: To assess the prevalence and associated factors of obesity in IBD.
Methods: We collected data about IBD disease pattern and activity, drugs and laboratory investigations in our center. Anthropometric measures were retrieved and obesity defined as a body mass index (BMI) > 30. Then, we compared characteristics of obese vs non obese patients, and Chi-squared test and Student's t test were used for discrete and continuous variables, respectively, at univariate analysis. For multivariate analysis, we used binomial logistic regression and estimated odd ratios (OR) and 95% confidence intervals (CI) to ascertain factors associated with obesity.
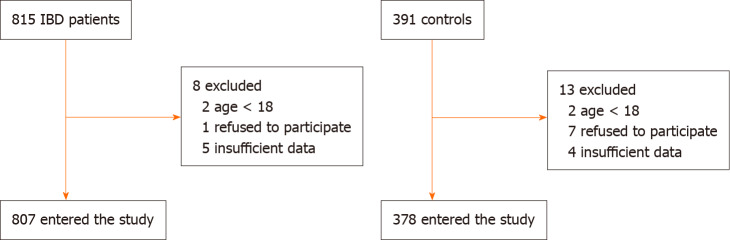
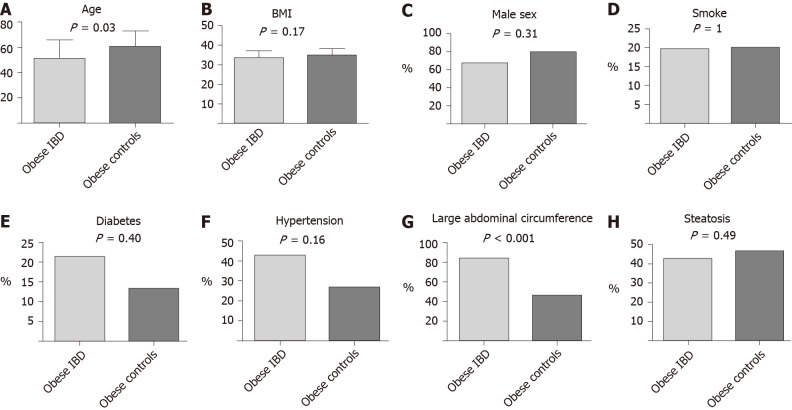
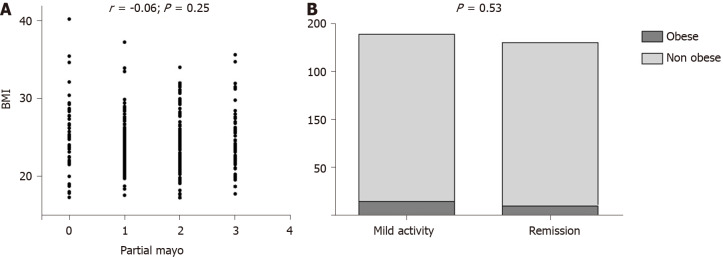
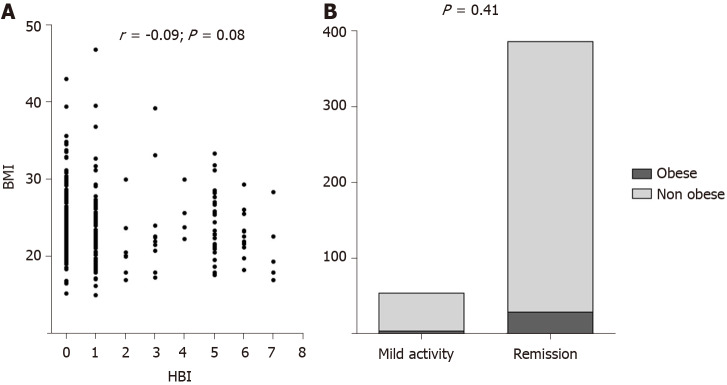
Results: We enrolled 807 patients with IBD, either ulcerative colitis (UC) or Crohn's disease (CD). Four hundred seventy-four patients were male (58.7%); the average age was 46.2 ± 13.2 years; 438 (54.2%) patients had CD and 369 (45.8%) UC. We enrolled 378 controls, who were comparable to IBD group for age, sex, BMI, obesity, diabetes and abdominal circumference, while more smokers and more subjects with hypertension were observed among controls. The prevalence of obesity was 6.9% in IBD and 7.9% in controls (not statistically different; P = 0.38). In the comparison of obese IBD patients and obese controls, we did not find any difference regarding diabetes and hypertension prevalence, nor in sex or smoking habits. Obese IBD patients were younger than obese controls (51.2 ± 14.9 years vs 60.7 ± 12.1 years, P = 0.03). At univariate analysis, obese IBD were older than normal weight ones (51.2 ± 14.9 vs 44.5 ± 15.8, P = 0.002). IBD onset age was earlier in obese population (44.8 ± 13.6 vs 35.6 ± 15.6, P = 0.004). We did not detect any difference in disease extension. Obese subjects had consumed more frequently long course of systemic steroids (66.6% vs 12.5%, P = 0.02) as well as antibiotics such as metronidazole or ciprofloxacin (71.4% vs 54.7%, P = 0.05). No difference about other drugs (biologics, mesalazine or thiopurines) was observed. Disease activity was similar between obese and non obese subjects both for UC and CD. Obese IBD patients suffered more frequently from arterial hypertension, type 2 diabetes, non-alcoholic fatty liver disease. Regarding laboratory investigations, obese IBD patients had higher levels of triglyceridemia, fasting blood glucose, gamma-glutamyl-transpeptidase. On multivariate analysis, however, the only factor that appeared to be independently linked to obesity in IBD was the high abdominal circumference (OR = 16.3, 95%CI: 1.03-250, P = 0.04).
Conclusion: Obese IBD patients seem to have features similar to general obese population, and there is no disease-specific factor (disease activity, extension or therapy) that may foster obesity in IBD.
Keywords: Antibiotics; Body mass index; Corticosteroids; Inflammatory bowel disease; Obesity; Risk factor.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Figures
References
-
- Yoon KH, Lee JH, Kim JW, Cho JH, Choi YH, Ko SH, Zimmet P, Son HY. Epidemic obesity and type 2 diabetes in Asia. Lancet. 2006;368:1681–1688. - PubMed
-
- Seravalle G, Grassi G. Obesity and hypertension. Pharmacol Res. 2017;122:1–7. - PubMed
-
- World Health Organization. Obesity. [cited April 13, 2020]. Available from: https://www.who.int/topics/obesity/en/
-
- Vadan R, Gheorghe LS, Constantinescu A, Gheorghe C. The prevalence of malnutrition and the evolution of nutritional status in patients with moderate to severe forms of Crohn's disease treated with Infliximab. Clin Nutr. 2011;30:86–91. - PubMed
-
- Blain A, Cattan S, Beaugerie L, Carbonnel F, Gendre JP, Cosnes J. Crohn's disease clinical course and severity in obese patients. Clin Nutr. 2002;21:51–57. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
