

Deep Sequencing of B Cell Receptor Repertoires From COVID-19 Patients Reveals Strong Convergent Immune Signatures
- PMID: 33384691
- PMCID: PMC7769841
- DOI: 10.3389/fimmu.2020.605170
Deep Sequencing of B Cell Receptor Repertoires From COVID-19 Patients Reveals Strong Convergent Immune Signatures
Abstract
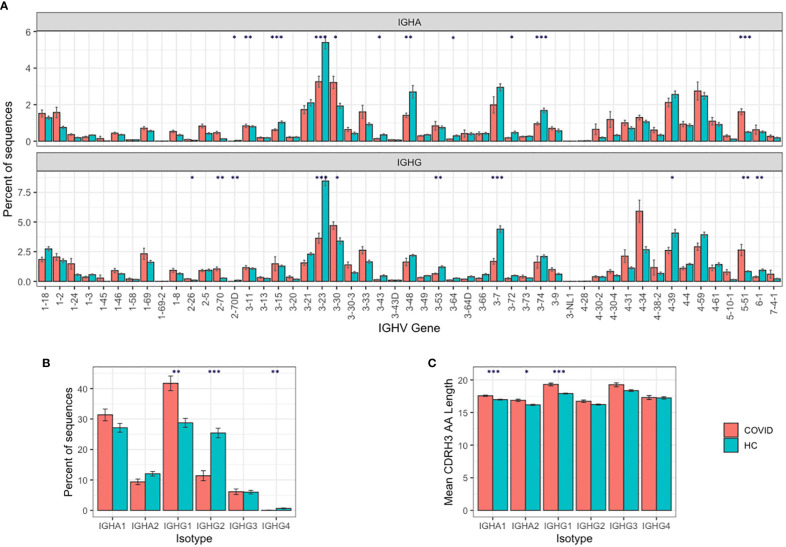
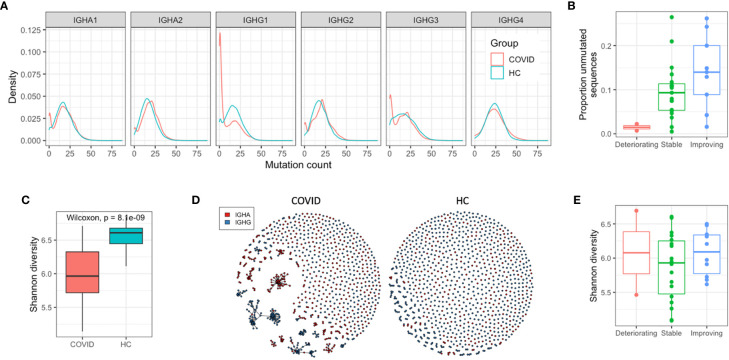
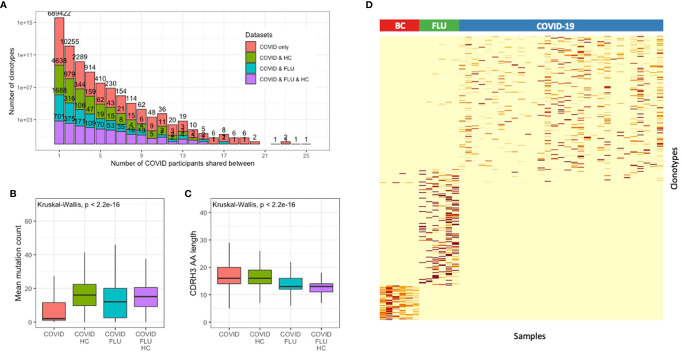
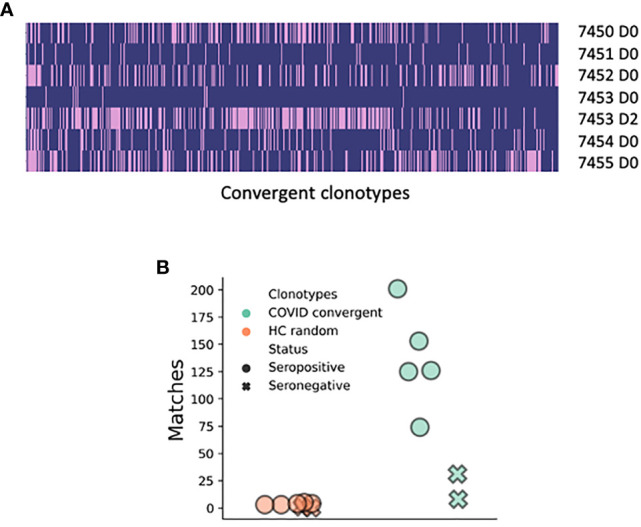
Deep sequencing of B cell receptor (BCR) heavy chains from a cohort of 31 COVID-19 patients from the UK reveals a stereotypical naive immune response to SARS-CoV-2 which is consistent across patients. Clonal expansion of the B cell population is also observed and may be the result of memory bystander effects. There was a strong convergent sequence signature across patients, and we identified 1,254 clonotypes convergent between at least four of the COVID-19 patients, but not present in healthy controls or individuals following seasonal influenza vaccination. A subset of the convergent clonotypes were homologous to known SARS and SARS-CoV-2 spike protein neutralizing antibodies. Convergence was also demonstrated across wide geographies by comparison of data sets between patients from UK, USA, and China, further validating the disease association and consistency of the stereotypical immune response even at the sequence level. These convergent clonotypes provide a resource to identify potential therapeutic and prophylactic antibodies and demonstrate the potential of BCR profiling as a tool to help understand patient responses.
Keywords: B-cell repertoire; BCR; COVID-19; SARS-CoV-2; antibody; convergence.
Copyright © 2020 Galson, Schaetzle, Bashford-Rogers, Raybould, Kovaltsuk, Kilpatrick, Minter, Finch, Dias, James, Thomas, Lee, Betley, Cavlan, Leech, Deane, Seoane, Caldas, Pennington, Pfeffer and Osbourn.
Conflict of interest statement
JO, AL, OC, SS, JG, JD, RM, and DF are employees of Alchemab Therapeutics Limited. RB-R is a founder of and consultant to Alchemab Therapeutics Limited. GK is a consultant to Alchemab Therapeutics Limited. CC is a member of the AstraZeneca External Science Panel and has research grants from Roche, Genentech, AstraZeneca, and Servier that are administered by the University of Cambridge. JB was employed by Illumina, Inc. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous