

Vasopressin in vasoplegic shock: A systematic review
- PMID: 33384951
- PMCID: PMC7754532
- DOI: 10.5492/wjccm.v9.i5.88
Vasopressin in vasoplegic shock: A systematic review
Abstract
Background: Vasoplegic shock is a challenging complication of cardiac surgery and is often resistant to conventional therapies for shock. Norepinephrine and epinephrine are standards of care for vasoplegic shock, but vasopressin has increasingly been used as a primary pressor in vasoplegic shock because of its unique pharmacology and lack of inotropic activity. It remains unclear whether vasopressin has distinct benefits over standard of care for patients with vasoplegic shock.
Aim: To summarize the available literature evaluating vasopressin vs non-vasopressin alternatives on the clinical and patient-centered outcomes of vasoplegic shock in adult intensive care unit (ICU) patients.
Methods: This was a systematic review of vasopressin in adults (≥ 18 years) with vasoplegic shock after cardiac surgery. Randomized controlled trials, prospective cohorts, and retrospective cohorts comparing vasopressin to norepinephrine, epinephrine, methylene blue, hydroxocobalamin, or other pressors were included. The primary outcomes of interest were 30-d mortality, atrial/ventricular arrhythmias, stroke, ICU length of stay, duration of vasopressor therapy, incidence of acute kidney injury stage II-III, and mechanical ventilation for greater than 48 h.
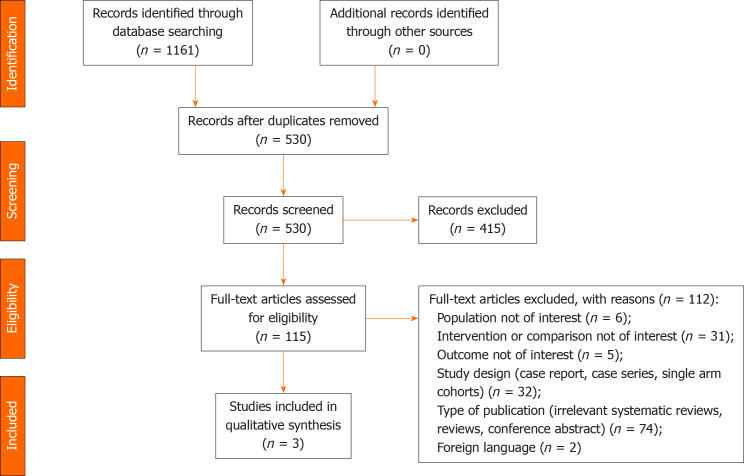
Results: A total of 1161 studies were screened for inclusion with 3 meeting inclusion criteria with a total of 708 patients. Two studies were randomized controlled trials and one was a retrospective cohort study. Primary outcomes of 30-d mortality, stroke, ventricular arrhythmias, and duration of mechanical ventilation were similar between groups. Conflicting results were observed for acute kidney injury stage II-III, atrial arrhythmias, duration of vasopressors, and ICU length of stay with higher certainty of evidence in favor of vasopressin serving a protective role for these outcomes.
Conclusion: Vasopressin was not found to be superior to alternative pressor therapy for any of the included outcomes. Results are limited by mixed methodologies, small overall sample size, and heterogenous populations.
Keywords: Arginine vasopressin; Shock; Treatment outcome; Vasoactive agents; Vasoplegia; Vasopressins.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have nothing to disclose.
Similar articles
-
Vasopressin in vasoplegic shock in surgical patients: systematic review and meta-analysis.Acta Cir Bras. 2023 Dec 1;38:e387523. doi: 10.1590/acb387523. eCollection 2023. Acta Cir Bras. 2023. PMID: 38055405 Free PMC article.
-
Evaluation of Vasopressin for Vasoplegic Shock in Patients With Preoperative Left Ventricular Dysfunction After Cardiac Surgery: A Propensity-Score Analysis.Shock. 2018 Nov;50(5):519-524. doi: 10.1097/SHK.0000000000001114. Shock. 2018. PMID: 29424795
-
Vasopressin versus Norepinephrine in Patients with Vasoplegic Shock after Cardiac Surgery: The VANCS Randomized Controlled Trial.Anesthesiology. 2017 Jan;126(1):85-93. doi: 10.1097/ALN.0000000000001434. Anesthesiology. 2017. PMID: 27841822 Clinical Trial.
-
Vasoplegic syndrome after cardiovascular surgery: A review of pathophysiology and outcome-oriented therapeutic management.J Card Surg. 2021 Oct;36(10):3749-3760. doi: 10.1111/jocs.15805. Epub 2021 Jul 12. J Card Surg. 2021. PMID: 34251716
-
CytoResc - "CytoSorb" Rescue for critically ill patients undergoing the COVID-19 Cytokine Storm: A structured summary of a study protocol for a randomized controlled trial.Trials. 2020 Jun 26;21(1):577. doi: 10.1186/s13063-020-04501-0. Trials. 2020. PMID: 32586396 Free PMC article.
Cited by
-
Hemodynamic Management with Vasopressin for Cardiovascular Surgery.Medicina (Kaunas). 2024 Dec 16;60(12):2064. doi: 10.3390/medicina60122064. Medicina (Kaunas). 2024. PMID: 39768943 Free PMC article. Review.
-
The Use of Methylene Blue during Liver Transplantation for Vasoplegia.Case Rep Anesthesiol. 2021 Jun 23;2021:6610754. doi: 10.1155/2021/6610754. eCollection 2021. Case Rep Anesthesiol. 2021. PMID: 34258070 Free PMC article.
-
Vasopressin in vasoplegic shock in surgical patients: systematic review and meta-analysis.Acta Cir Bras. 2023 Dec 1;38:e387523. doi: 10.1590/acb387523. eCollection 2023. Acta Cir Bras. 2023. PMID: 38055405 Free PMC article.
References
-
- Mekontso-Dessap A, Houël R, Soustelle C, Kirsch M, Thébert D, Loisance DY. Risk factors for post-cardiopulmonary bypass vasoplegia in patients with preserved left ventricular function. Ann Thorac Surg. 2001;71:1428–1432. - PubMed
-
- Levin MA, Lin HM, Castillo JG, Adams DH, Reich DL, Fischer GW. Early on-cardiopulmonary bypass hypotension and other factors associated with vasoplegic syndrome. Circulation. 2009;120:1664–1671. - PubMed
-
- Kohl BA, Deutschman CS. The inflammatory response to surgery and trauma. Curr Opin Crit Care. 2006;12:325–332. - PubMed
-
- Sun X, Zhang L, Hill PC, Lowery R, Lee AT, Molyneaux RE, Corso PJ, Boyce SW. Is incidence of postoperative vasoplegic syndrome different between off-pump and on-pump coronary artery bypass grafting surgery? Eur J Cardiothorac Surg. 2008;34:820–825. - PubMed
LinkOut - more resources
Full Text Sources
