

Coronary Artery Calcium Scoring: New Insights into Clinical Interpretation-Lessons from the CAC Consortium
- PMID: 33385165
- PMCID: PMC7757721
- DOI: 10.1148/ryct.2020200281
Coronary Artery Calcium Scoring: New Insights into Clinical Interpretation-Lessons from the CAC Consortium
Abstract
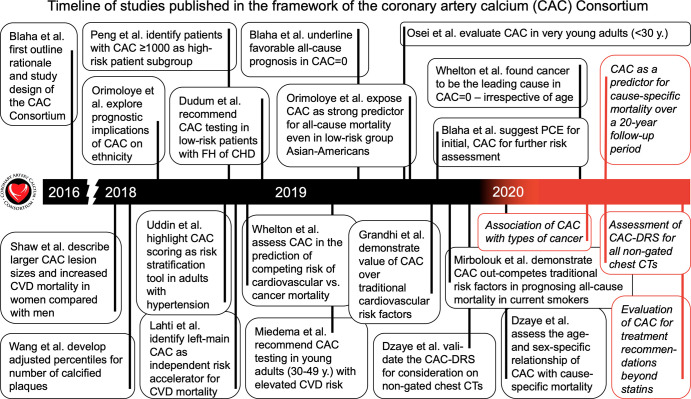
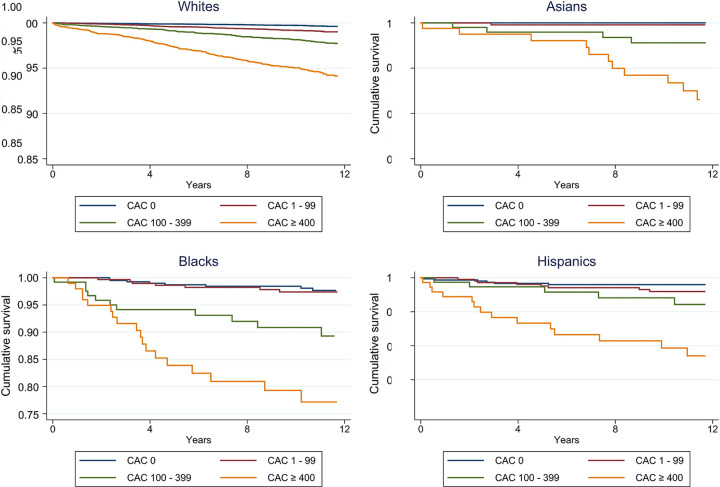
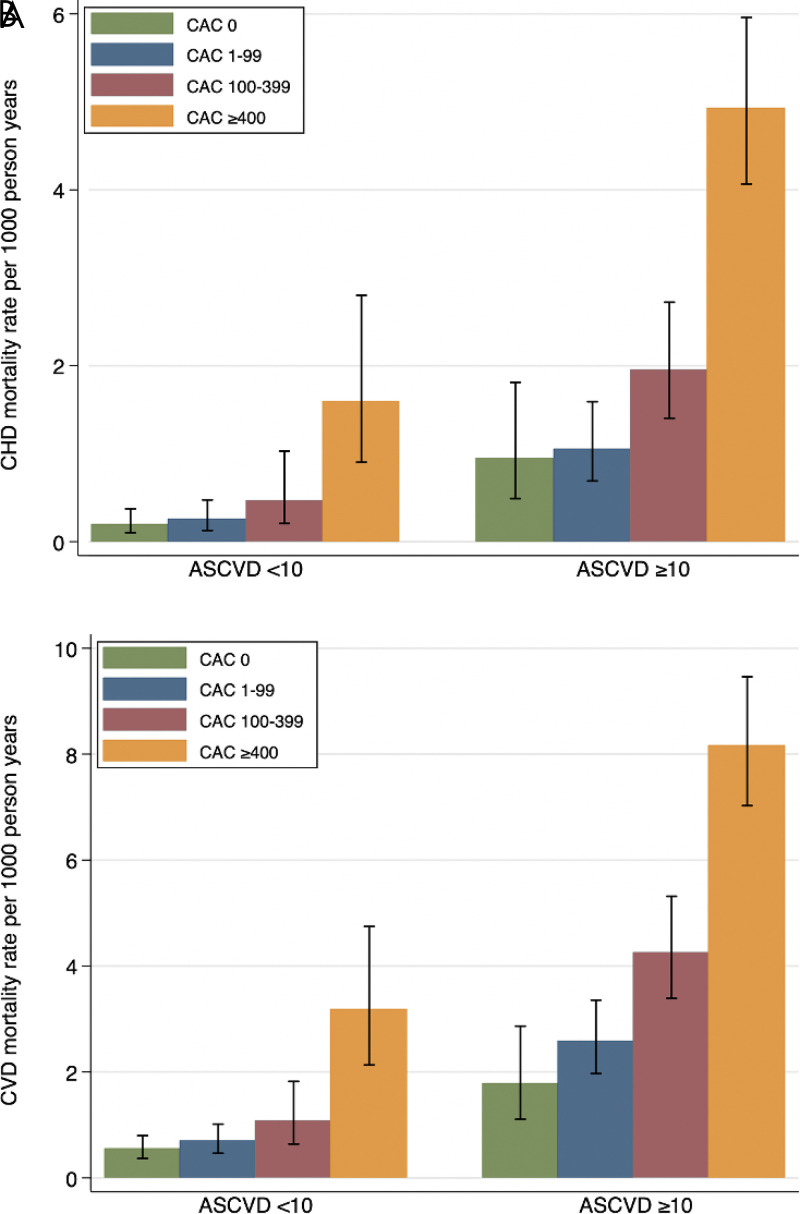
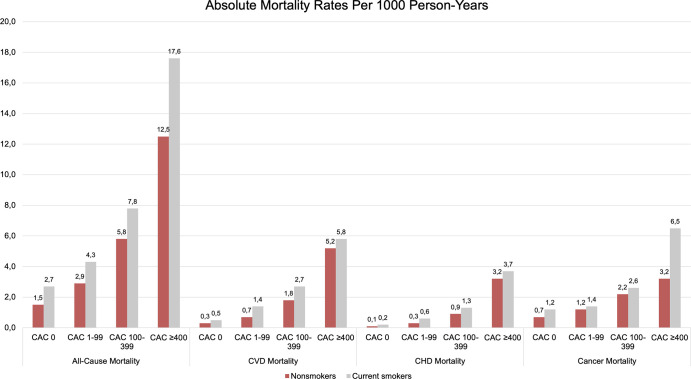
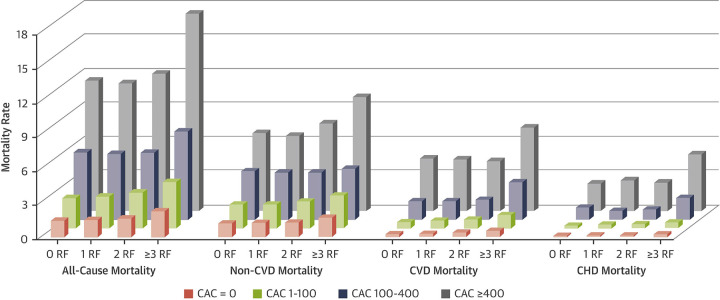
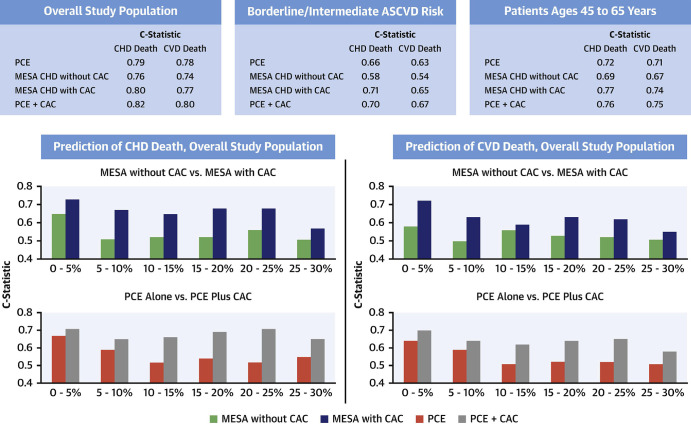
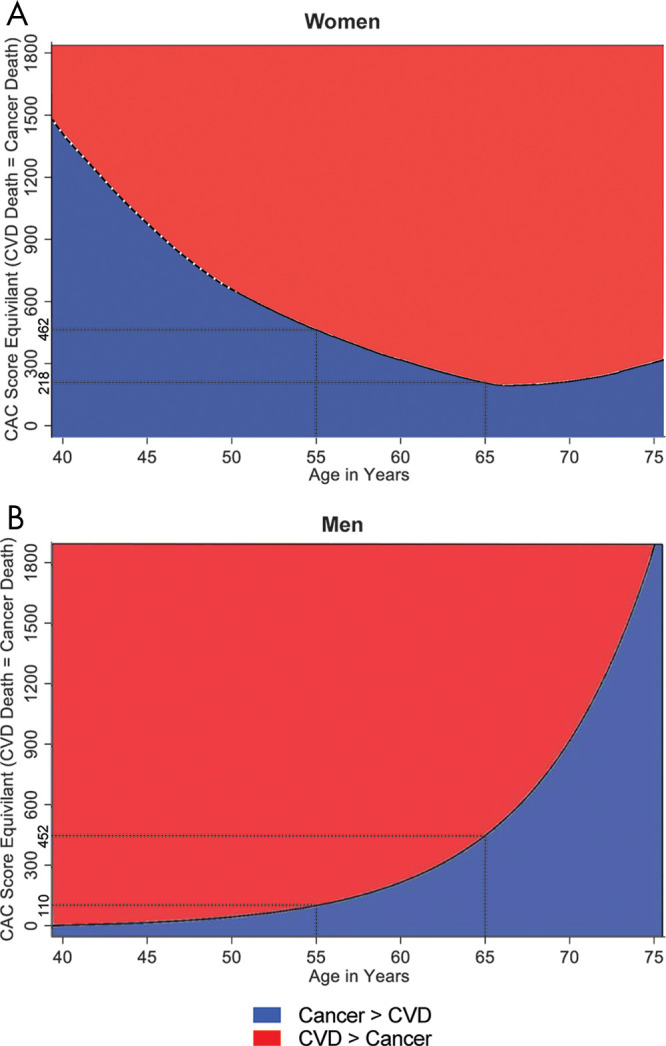
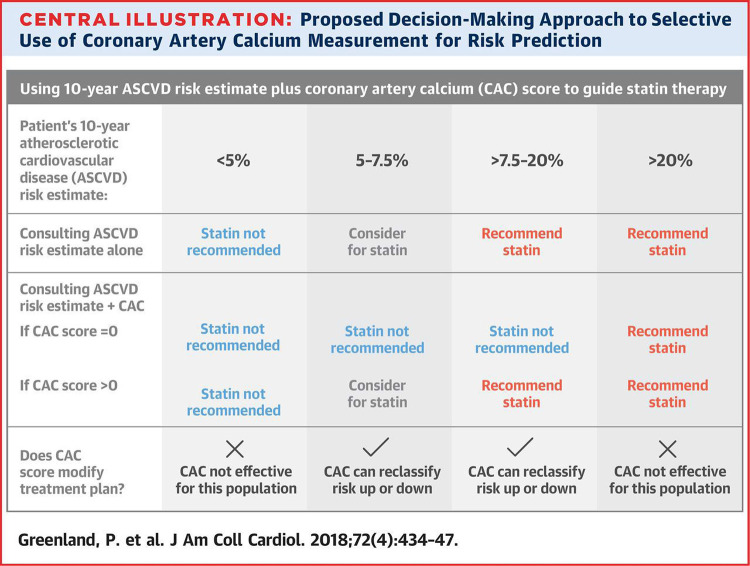
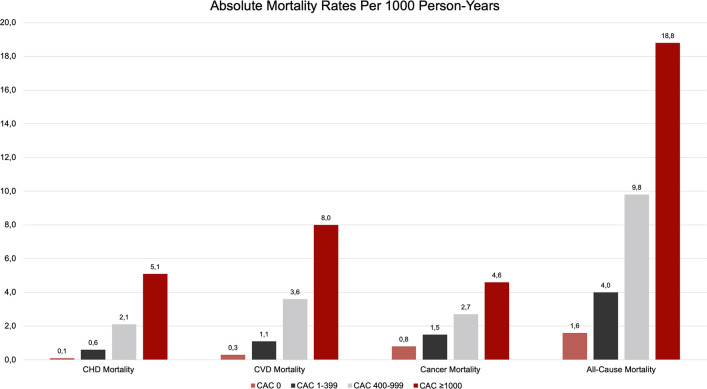
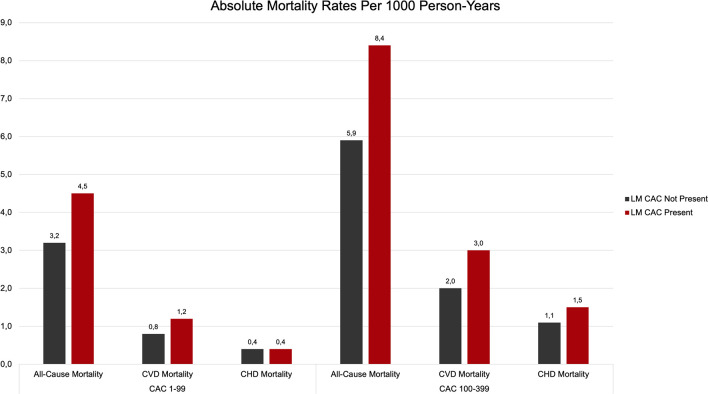
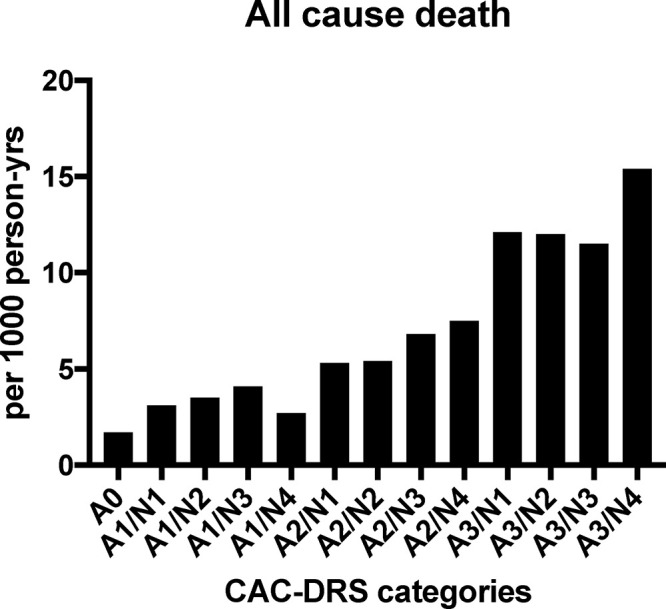
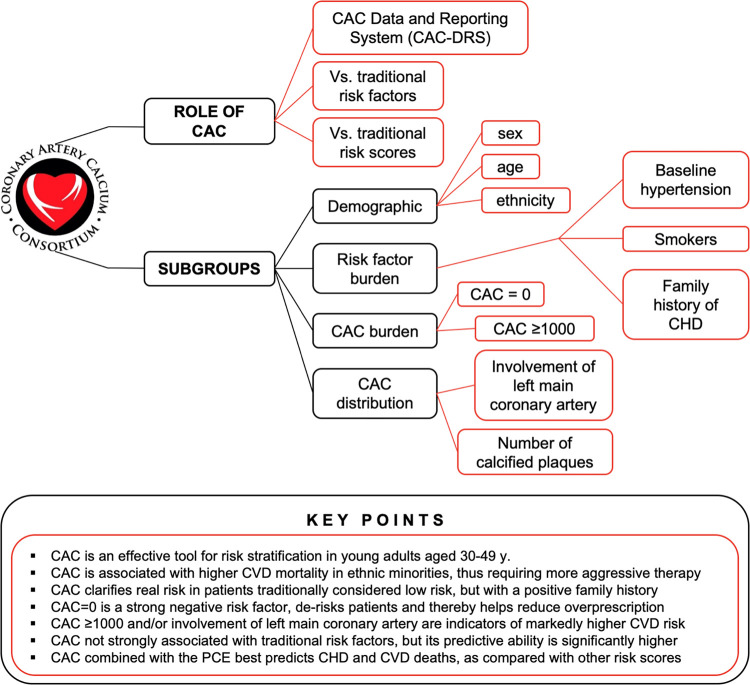
Coronary artery calcium (CAC) is a highly specific marker for coronary atherosclerosis. The CAC Consortium, a multicenter, retrospective, real-world cohort study, was established to investigate the association between CAC and long-term, cause-specific mortality. This review summarizes findings from CAC Consortium studies published between 2016 and 2020, aiming to demystify CAC as a clinical decision-guiding tool and push the limits of who might benefit from CAC in clinical practice. CAC has been shown to effectively stratify cardiovascular risk across ethnicities irrespective of age, sex, and risk factor burden. In comparison to other widely used risk scores, CAC appears to be most consistent in its ability to add to cardiovascular disease (CVD) event prediction. Beyond risk stratification, CAC has been shown to identify high-risk patient subgroups. While currently recommended only for patients at borderline or intermediate risk by the American College of Cardiology/American Heart Association (10-year atherosclerotic CVD event risk, 5% to < 20%), CAC scoring may also provide value in select young patients aged 30-49 years and in low-risk patients with a family history. While new studies emphasize that patients with a CAC greater than or equal to 1000 be considered a distinct patient group, a CAC of 0 has additionally emerged to be a reliable negative risk factor, identifying patients at low risk of both CVD and non-CVD mortality. © RSNA, 2020.
2020 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of Conflicts of Interest: S.A. disclosed no relevant relationships. S.M.I.U. disclosed no relevant relationships. A.D.O. disclosed no relevant relationships. O.H.O. disclosed no relevant relationships. M.J.B. Activities related to the present article: disclosed money paid to author’s institution from National Institutes of Health (NIH)/National Heart, Lung, and Blood Institute (NHLBI). Activities not related to the present article: disclosed money paid to author from Amgen, Sanofi, Regeneron, Novartis, Novo Nordisk, Bayer, Gilead, Zogenix, and Tricida for consultancy, advisory board, and mock AdCom preparation; disclosed grants/grants pending to author’s institution from NIH/NHLBI, Food and Drug Administration, American Heart Association, Aetna Foundation, and Amgen Foundation. Other relationships: disclosed no relevant relationships. O.D. disclosed no relevant relationships.
Figures
References
-
- Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990;15(4):827–832. - PubMed
-
- Bild DE, Bluemke DA, Burke GL, et al. Multi-Ethnic Study of Atherosclerosis: objectives and design. Am J Epidemiol 2002;156(9):871–881. - PubMed
-
- Schmermund A, Möhlenkamp S, Stang A, et al. Assessment of clinically silent atherosclerotic disease and established and novel risk factors for predicting myocardial infarction and cardiac death in healthy middle-aged subjects: rationale and design of the Heinz Nixdorf RECALL Study. Risk Factors, Evaluation of Coronary Calcium and Lifestyle. Am Heart J 2002;144(2):212–218. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
