

The Use of Acute Normovolemic Hemodilution in Clipping Surgery for Aneurysmal Subarachnoid Hemorrhage
- PMID: 33385596
- PMCID: PMC9760483
- DOI: 10.1016/j.wneu.2020.12.110
The Use of Acute Normovolemic Hemodilution in Clipping Surgery for Aneurysmal Subarachnoid Hemorrhage
Abstract
Background: The occurrence of coronavirus disease 2019 (COVID-19) has overwhelmed the blood supply chain worldwide and severely influenced clinical procedures with potential massive blood loss, such as clipping surgery for aneurysmal subarachnoid hemorrhage (aSAH). Whether acute normovolemic hemodilution (ANH) is safe and effective in aneurysm clipping remains largely unknown.
Methods: Patients with aSAH who underwent clipping surgery within 72 hours from bleeding were included. The patients in the ANH group received 400 mL autologous blood collection, and the blood was returned as needed during surgery. The relationships between ANH and perioperative allogeneic blood transfusion, postoperative outcome, and complications were analyzed.
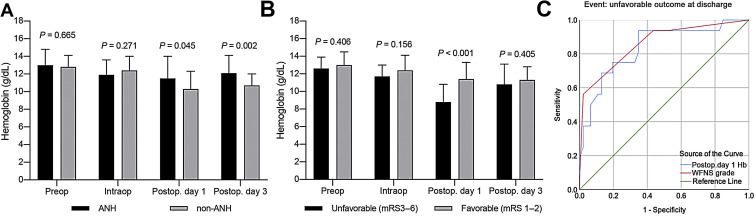
Results: Sixty-two patients with aSAH were included between December 2019 and June 2020 (20 in the ANH group and 42 in the non-ANH group). ANH did not reduce the need of perioperative blood transfusion (3 [15%] vs. 5 [11.9%]; P = 0.734). However, ANH significantly increased serum hemoglobin levels on postoperative day 1 (11.5 ± 2.5 g/dL vs. 10.3 ± 2.0 g/dL; P = 0.045) and day 3 (12.1 ± 2.0 g/dL vs. 10.7 ± 1.3 g/dL; P = 0.002). Multivariable analysis indicated that serum hemoglobin level on postoperative day 1 (odds ratio, 0.895; 95% confidence interval, 0.822-0.973; P = 0.010) was an independent risk factor for unfavorable outcome, and receiver operating characteristic curve analysis showed that it had a comparable predictive power to World Federation of Neurosurgical Societies grade (Z = 0.275; P > 0.05).
Conclusions: ANH significantly increased postoperative hemoglobin levels, and it may hold the potential to improve patients' outcomes. Routine use of ANH should be considered in aneurysm clipping surgery.
Keywords: Acute normovolemic hemodilution; Clipping; Functional outcome; Subarachnoid hemorrhage.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Acute normovolemic hemodilution is safe in neurosurgery.World Neurosurg. 2013 May-Jun;79(5-6):719-24. doi: 10.1016/j.wneu.2012.02.041. Epub 2012 Feb 13. World Neurosurg. 2013. PMID: 22381828 Clinical Trial.
-
Outcome After Clipping and Coiling for Aneurysmal Subarachnoid Hemorrhage in Clinical Practice in Europe, USA, and Australia.Neurosurgery. 2019 May 1;84(5):1019-1027. doi: 10.1093/neuros/nyy223. Neurosurgery. 2019. PMID: 29846713 Free PMC article.
-
A prospective randomized trial of acute normovolemic hemodilution compared to standard intraoperative management in patients undergoing major hepatic resection.Ann Surg. 2008 Sep;248(3):360-9. doi: 10.1097/SLA.0b013e318184db08. Ann Surg. 2008. PMID: 18791356 Clinical Trial.
-
Effect of acute normovolemic hemodilution on coronary artery bypass grafting: A systematic review and meta-analysis of 22 randomized trials.Int J Surg. 2020 Nov;83:131-139. doi: 10.1016/j.ijsu.2020.09.016. Epub 2020 Sep 18. Int J Surg. 2020. PMID: 32950743
-
Endovascular coiling versus neurosurgical clipping for people with aneurysmal subarachnoid haemorrhage.Cochrane Database Syst Rev. 2018 Aug 15;8(8):CD003085. doi: 10.1002/14651858.CD003085.pub3. Cochrane Database Syst Rev. 2018. PMID: 30110521 Free PMC article.
Cited by
-
Hematocrit drift and outcomes in surgical patients with aneurysmal subarachnoid hemorrhage.Acta Neurochir (Wien). 2024 May 4;166(1):202. doi: 10.1007/s00701-024-06097-9. Acta Neurochir (Wien). 2024. PMID: 38703244
-
Development and validation of a nomogram for blood transfusion during intracranial aneurysm clamping surgery: a retrospective analysis.BMC Med Inform Decis Mak. 2023 Apr 19;23(1):71. doi: 10.1186/s12911-023-02157-9. BMC Med Inform Decis Mak. 2023. PMID: 37076865 Free PMC article.
-
Systematic review and meta-analysis of outcome-relevant anemia in patients with subarachnoid hemorrhage.Sci Rep. 2022 Dec 1;12(1):20738. doi: 10.1038/s41598-022-24591-x. Sci Rep. 2022. PMID: 36456587 Free PMC article.
References
-
- Macdonald R.L., Schweizer T.A. Spontaneous subarachnoid haemorrhage. Lancet. 2017;389:655–666. - PubMed
-
- Lin Q.S., Wang W.X., Lin Y.X., et al. Annexin A7 induction of neuronal apoptosis via effect on glutamate release in a rat model of subarachnoid hemorrhage. J Neurosurg. 2020;132:777–787. - PubMed
-
- Connolly E.S., Jr., Rabinstein A.A., Carhuapoma J.R., et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke. 2012;43:1711–1737. - PubMed
-
- Kumar M.A., Levine J., Faerber J., et al. The effects of red blood cell transfusion on functional outcome after aneurysmal subarachnoid hemorrhage. World Neurosurg. 2017;108:807–816. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
