

Anthracycline-induced cytotoxicity in the GL261 glioma model system
- PMID: 33387196
- PMCID: PMC7884566
- DOI: 10.1007/s11033-020-06109-8
Anthracycline-induced cytotoxicity in the GL261 glioma model system
Abstract
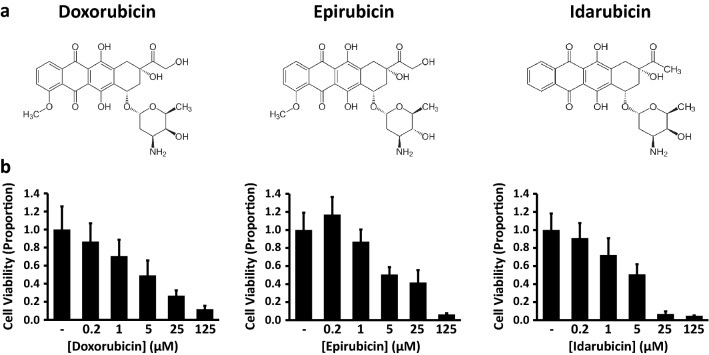
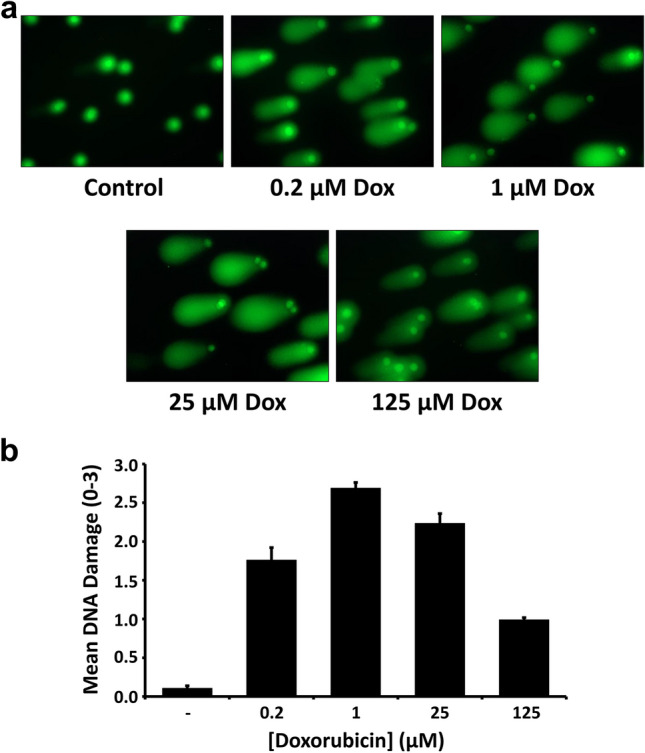
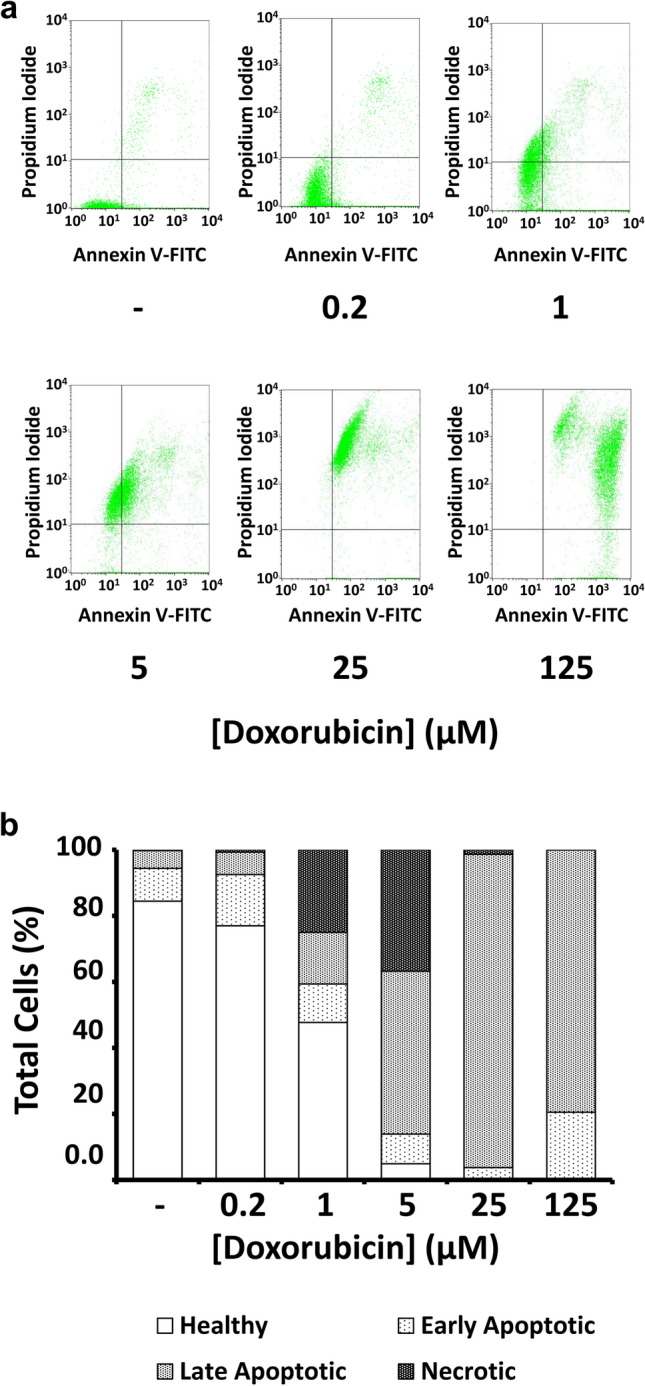
Glioblastoma (GBM) is a lethal astrocyte-derived tumor that is currently treated with a multi-modal approach of surgical resection, radiotherapy, and temozolomide-based chemotherapy. Alternatives to current therapies are urgently needed as its prognosis remains poor. Anthracyclines are a class of compounds that show great potential as GBM chemotherapeutic agents and are widely used to treat solid tumors outside the central nervous system. Here we investigate the cytotoxic effects of doxorubicin and other anthracyclines on GL261 glioma tumor cells in anticipation of novel anthracycline-based CNS therapies. Three methods were used to quantify dose-dependent effects of anthracyclines on adherent GL261 tumor cells, a murine cell-based model of GBM. MTT assays quantified anthracycline effects on cell viability, comet assays examined doxorubicin genotoxicity, and flow cytometry with Annexin V/PI staining characterized doxorubicin-induced apoptosis and necrosis. Dose-dependent reductions in GL261 cell viability were found in cells treated with doxorubicin (EC50 = 4.9 μM), epirubicin (EC50 = 5.9 μM), and idarubicin (EC50 = 4.4 μM). Comet assays showed DNA damage following doxorubicin treatments, peaking at concentrations of 1.0 μM and declining after 25 μM. Lastly, flow cytometric analysis of doxorubicin-treated cells showed dose-dependent induction of apoptosis (EC50 = 5.2 μM). Together, these results characterized the cytotoxic effects of anthracyclines on GL261 glioma cells. We found dose-dependent apoptotic induction; however at high concentrations we find that cell death is likely necrotic. Our results support the continued exploration of anthracyclines as compounds with significant potential for improved GBM treatments.
Keywords: Comet assay; Doxorubicin; Flow cytometry; GL261; Glioblastoma; MTT.
Conflict of interest statement
The authors have no competing interests to declare.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
