

The effects of a family-centered psychosocial-based nutrition intervention in patients with advanced cancer: the PiCNIC2 pilot randomised controlled trial
- PMID: 33388075
- PMCID: PMC7778804
- DOI: 10.1186/s12937-020-00657-2
The effects of a family-centered psychosocial-based nutrition intervention in patients with advanced cancer: the PiCNIC2 pilot randomised controlled trial
Abstract
Background: Malnutrition in advanced cancer patients is common but limited and inconclusive data exists on the effectiveness of nutrition interventions. Feasibility and acceptability of a novel family-based nutritional psychosocial intervention were established recently. The aims of this present study were to assess the feasibility of undertaking a randomised controlled trial of the latter intervention, to pilot test outcome measures and to explore preliminary outcomes.
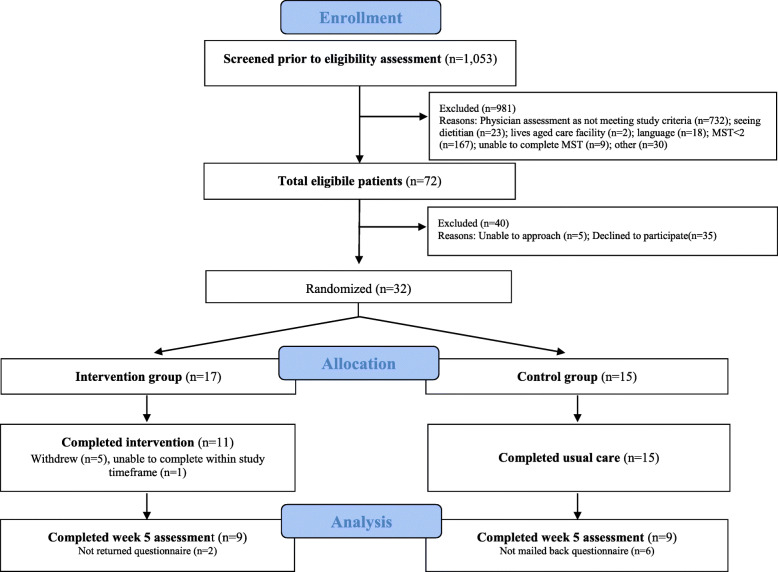
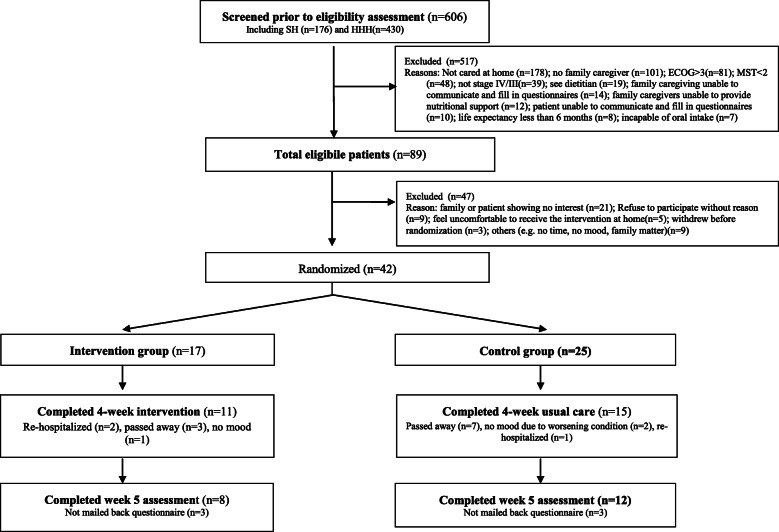
Methods: Pilot randomised controlled trial recruiting advanced cancer patients and family caregivers in Australia and Hong Kong. Participants were randomised and assigned to one of two groups, either a family-centered nutritional intervention or the control group receiving usual care only. The intervention provided 2-3 h of direct dietitian contact time with patients and family members over a 4-6-week period. During the intervention, issues with nutrition impact symptoms and food or eating-related psychosocial concerns were addressed through nutrition counselling, with a focus on improving nutrition-related communication between the dyads and setting nutritional goals. Feasibility assessment included recruitment, consent rate, retention rate, and acceptability of assessment tools. Validated nutritional and quality of life self-reported measures were used to collect patient and caregiver outcome data, including the 3-day food diary, the Patient-Generated Subjective Global Assessment Short Form, the Functional Assessment Anorexia/Cachexia scale, Eating-related Distress or Enjoyment, and measures of self-efficacy, carers' distress, anxiety and depression.
Results: Seventy-four patients and 54 family caregivers participated in the study. Recruitment was challenging, and for every patient agreeing to participate, 14-31 patients had to be screened. The consent rate was 44% in patients and 55% in caregivers. Only half the participants completed the trial's final assessment. The data showed promise for some patient outcomes in the intervention group, particularly with improvements in eating-related distress (p = 0.046 in the Australian data; p = 0.07 in the Hong Kong data), eating-related enjoyment (p = 0.024, Hong Kong data) and quality of life (p = 0.045, Australian data). Energy and protein intake also increased in a clinically meaningful way. Caregiver data on eating-related distress, anxiety, depression and caregiving burden, however, showed little or no change.
Conclusions: Despite challenges with participant recruitment, the intervention demonstrates good potential to have positive effects on patients' nutritional status and eating-related distress. The results of this trial warrant a larger and fully-powered trial to ascertain the effectiveness of this intervention.
Trial registration: The trial was registered with the Australian & New Zealand Clinical Trials Registry, registration number ACTRN12618001352291 .
Keywords: Advanced cancer; Anorexia; Caregivers; Eating-related distress; Malnutrition; Quality of life.
Conflict of interest statement
We declare no competing interests by any of the authors.
Figures
References
-
- Aktas A, Walsh D, Galang M, O’Donoghue N, Rybicki L, Hullihen B, Schleckman E. Underrecognition of Malnutrition in Advanced Cancer The Role of the Dietitian and Clinical Practice Variations. Am J Hosp Palliat Med. 2016. 10.1177/1049909116639969. - PubMed
-
- Amano K, Maeda I, Morita T, Okajima Y, Hama T, Aoyama M, et al. Eating-related distress and need for nutritional support of families of advanced cancer patients: a nationwide survey of bereaved family members. J Cachexia Sarcopenia Muscle. 2016;7(5):527–534. doi: 10.1002/jcsm.12102. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
