

Colonic Epithelial-Derived Selenoprotein P Is the Source for Antioxidant-Mediated Protection in Colitis-Associated Cancer
- PMID: 33388316
- PMCID: PMC8035252
- DOI: 10.1053/j.gastro.2020.12.059
Colonic Epithelial-Derived Selenoprotein P Is the Source for Antioxidant-Mediated Protection in Colitis-Associated Cancer
Abstract
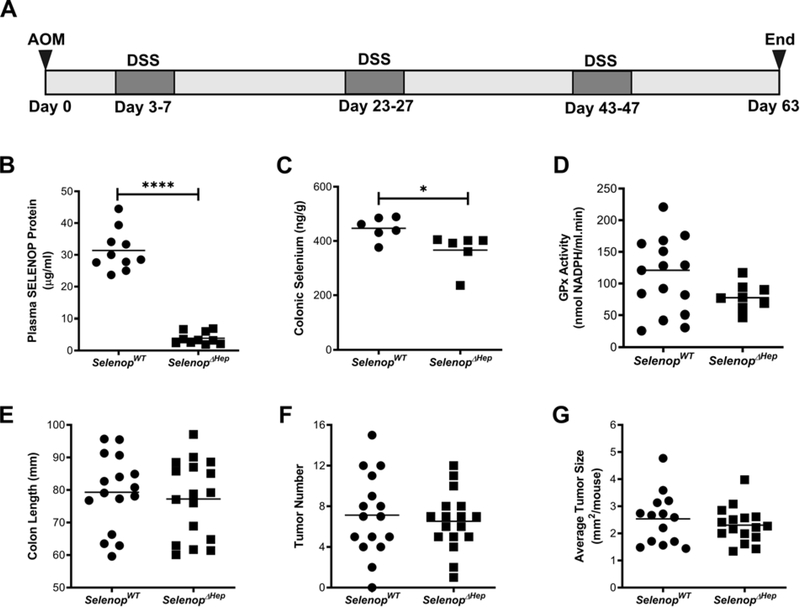
Background & aims: Patients with inflammatory bowel disease (IBD) demonstrate nutritional selenium deficiencies and are at greater risk of developing colon cancer. Previously, we determined that global reduction of the secreted antioxidant selenium-containing protein, selenoprotein P (SELENOP), substantially increased tumor development in an experimental colitis-associated cancer (CAC) model. We next sought to delineate tissue-specific contributions of SELENOP to intestinal inflammatory carcinogenesis and define clinical context.
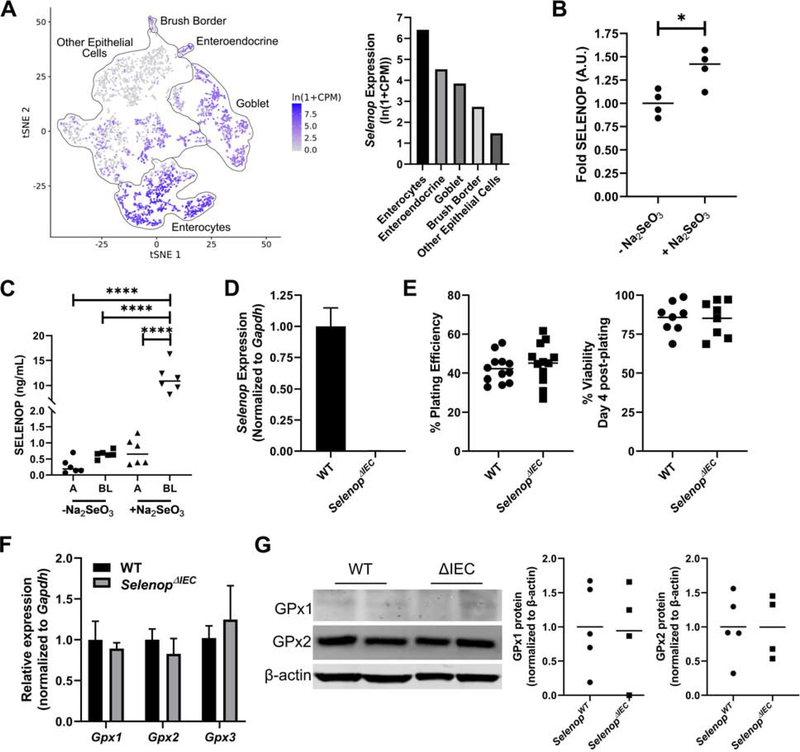
Methods: Selenop floxed mice crossed with Cre driver lines to delete Selenop from the liver, myeloid lineages, or intestinal epithelium were placed on an azoxymethane/dextran sodium sulfate experimental CAC protocol. SELENOP loss was assessed in human ulcerative colitis (UC) organoids, and expression was queried in human and adult UC samples.
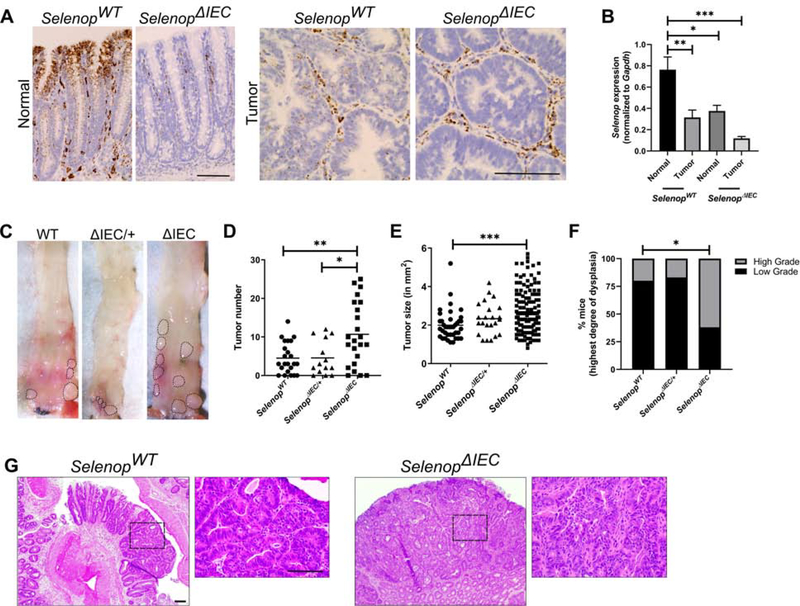
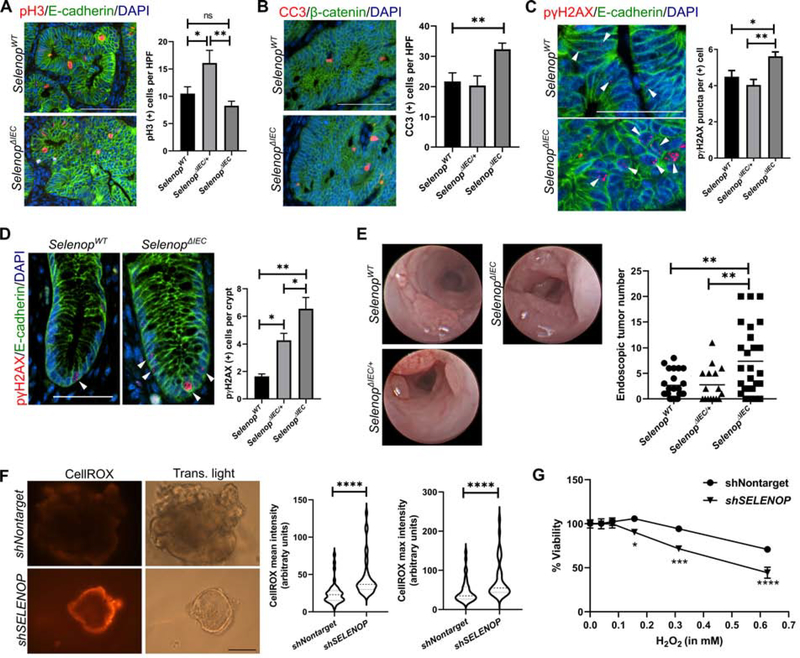
Results: Although large sources of SELENOP, both liver- and myeloid-specific Selenop deletion failed to modify azoxymethane/dextran sodium sulfate-mediated tumorigenesis. Instead, epithelial-specific deletion increased CAC tumorigenesis, likely due to elevated oxidative stress with a resulting increase in genomic instability and augmented tumor initiation. SELENOP was down-regulated in UC colon biopsies and levels were inversely correlated with endoscopic disease severity and tissue S100A8 (calprotectin) gene expression.
Conclusions: Although global selenium status is typically assessed by measuring liver-derived plasma SELENOP levels, our results indicate that the peripheral SELENOP pool is dispensable for CAC. Colonic epithelial SELENOP is the main contributor to local antioxidant capabilities. Thus, colonic SELENOP is the most informative means to assess selenium levels and activity in IBD patients and may serve as a novel biomarker for UC disease severity and identify patients most predisposed to CAC development.
Keywords: Colitis-Associated Cancer; Reactive Oxygen Species; Selenium; Selenoproteins.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures



References
-
- Baum MK, Shor-Posner G, Lai S, et al. High risk of HIV-related mortality is associated with selenium deficiency. J Acquir Immune Defic Syndr Hum Retrovirol 1997;15:370–4. - PubMed
-
- Beck MA, Williams-Toone D, Levander OA. Coxsackievirus B3-resistant mice become susceptible in Se/vitamin E deficiency. Free Radic Biol Med 2003;34:1263–70. - PubMed
-
- Beck MA, Shi Q, Morris VC, et al. Rapid genomic evolution of a non-virulent coxsackievirus B3 in selenium-deficient mice results in selection of identical virulent isolates. Nat Med 1995;1:433–6. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
- R01 DK128200/DK/NIDDK NIH HHS/United States
- K01 DK123495/DK/NIDDK NIH HHS/United States
- R01 DK099204/DK/NIDDK NIH HHS/United States
- P30 DK058404/DK/NIDDK NIH HHS/United States
- F31 CA232272/CA/NCI NIH HHS/United States
- R01 DK117119/DK/NIDDK NIH HHS/United States
- U01 DK095745/DK/NIDDK NIH HHS/United States
- T32 GM152284/GM/NIGMS NIH HHS/United States
- F32 DK108492/DK/NIDDK NIH HHS/United States
- F31 CA167920/CA/NCI NIH HHS/United States
- R01 AT004821/AT/NCCIH NIH HHS/United States
- F30 DK103498/DK/NIDDK NIH HHS/United States
- T32 GM007347/GM/NIGMS NIH HHS/United States
- I01 BX001453/BX/BLRD VA/United States
- P30 CA068485/CA/NCI NIH HHS/United States
- I01 BX001426/BX/BLRD VA/United States
- I01 CX002171/CX/CSRD VA/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
