

Characterization of the Immune Landscape of EGFR-Mutant NSCLC Identifies CD73/Adenosine Pathway as a Potential Therapeutic Target
- PMID: 33388477
- PMCID: PMC11160459
- DOI: 10.1016/j.jtho.2020.12.010
Characterization of the Immune Landscape of EGFR-Mutant NSCLC Identifies CD73/Adenosine Pathway as a Potential Therapeutic Target
Abstract
Introduction: Lung adenocarcinomas harboring EGFR mutations do not respond to immune checkpoint blockade therapy and their EGFR wildtype counterpart. The mechanisms underlying this lack of clinical response have been investigated but remain incompletely understood.
Methods: We analyzed three cohorts of resected lung adenocarcinomas (Profiling of Resistance Patterns of Oncogenic Signaling Pathways in Evaluation of Cancer of Thorax, Immune Genomic Profiling of NSCLC, and The Cancer Genome Atlas) and compared tumor immune microenvironment of EGFR-mutant tumors to EGFR wildtype tumors, to identify actionable regulators to target and potentially enhance the treatment response.
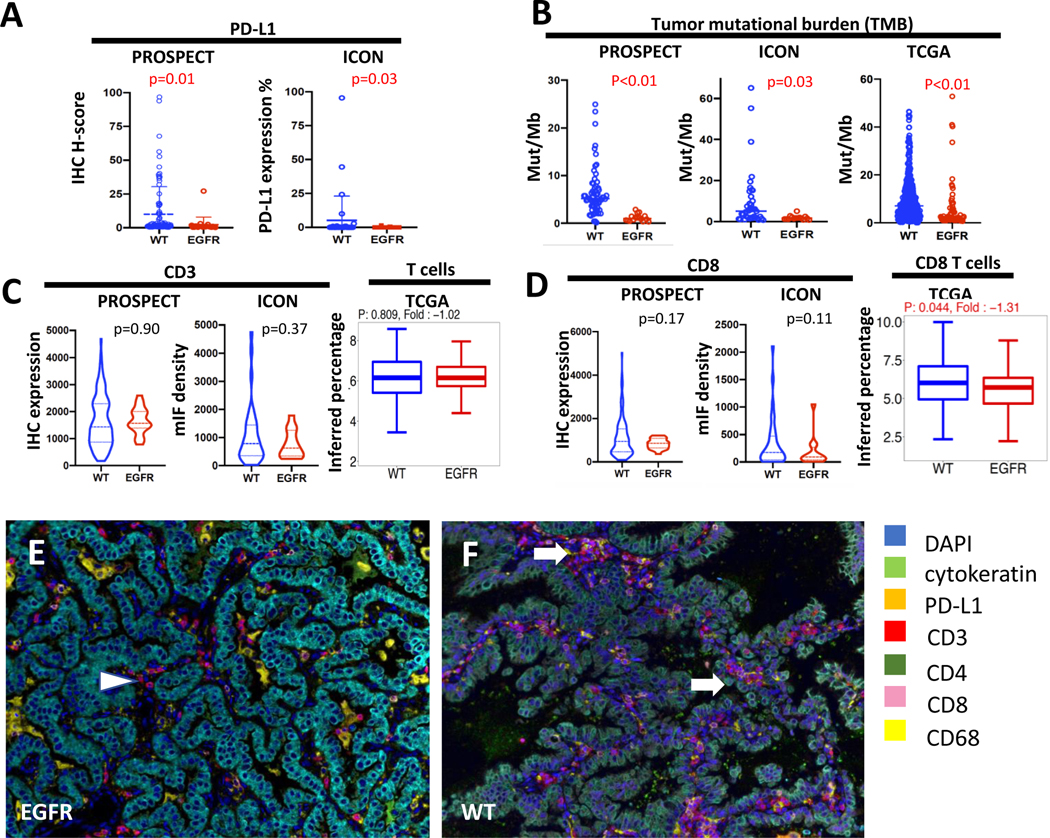
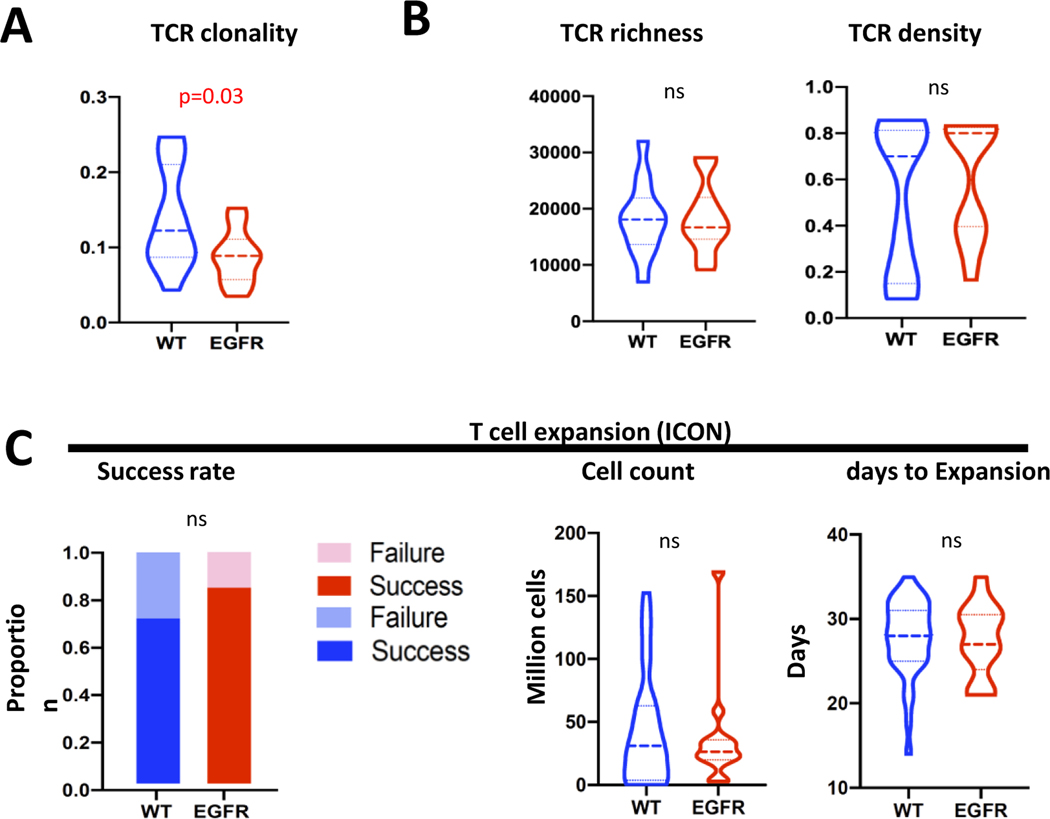
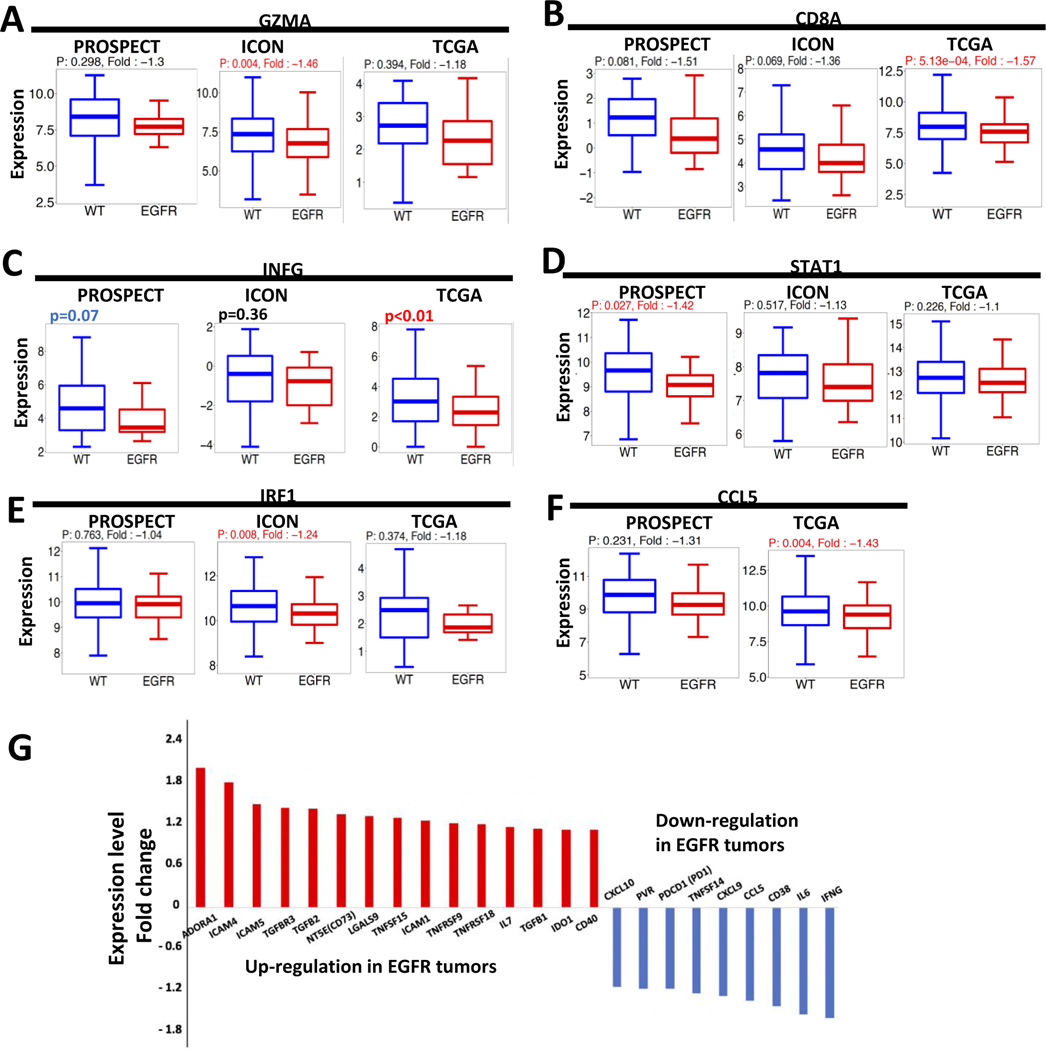
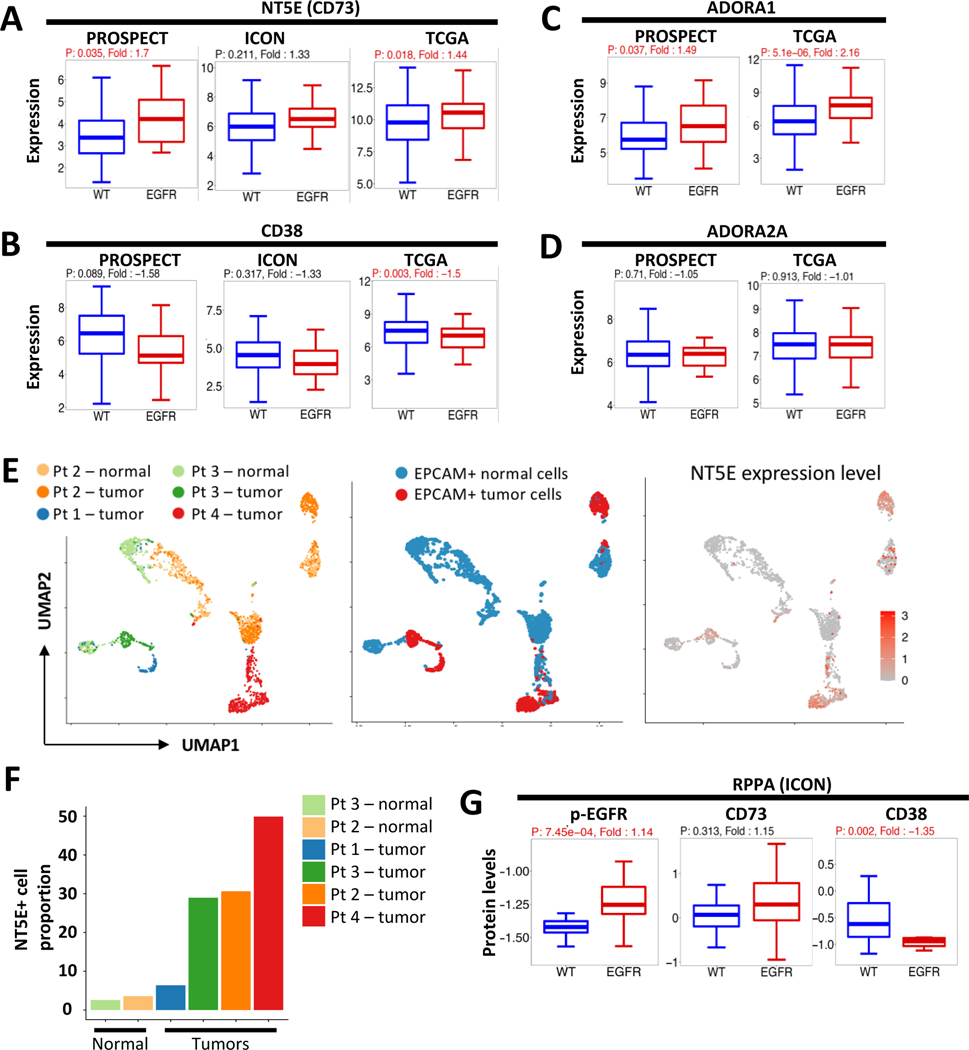
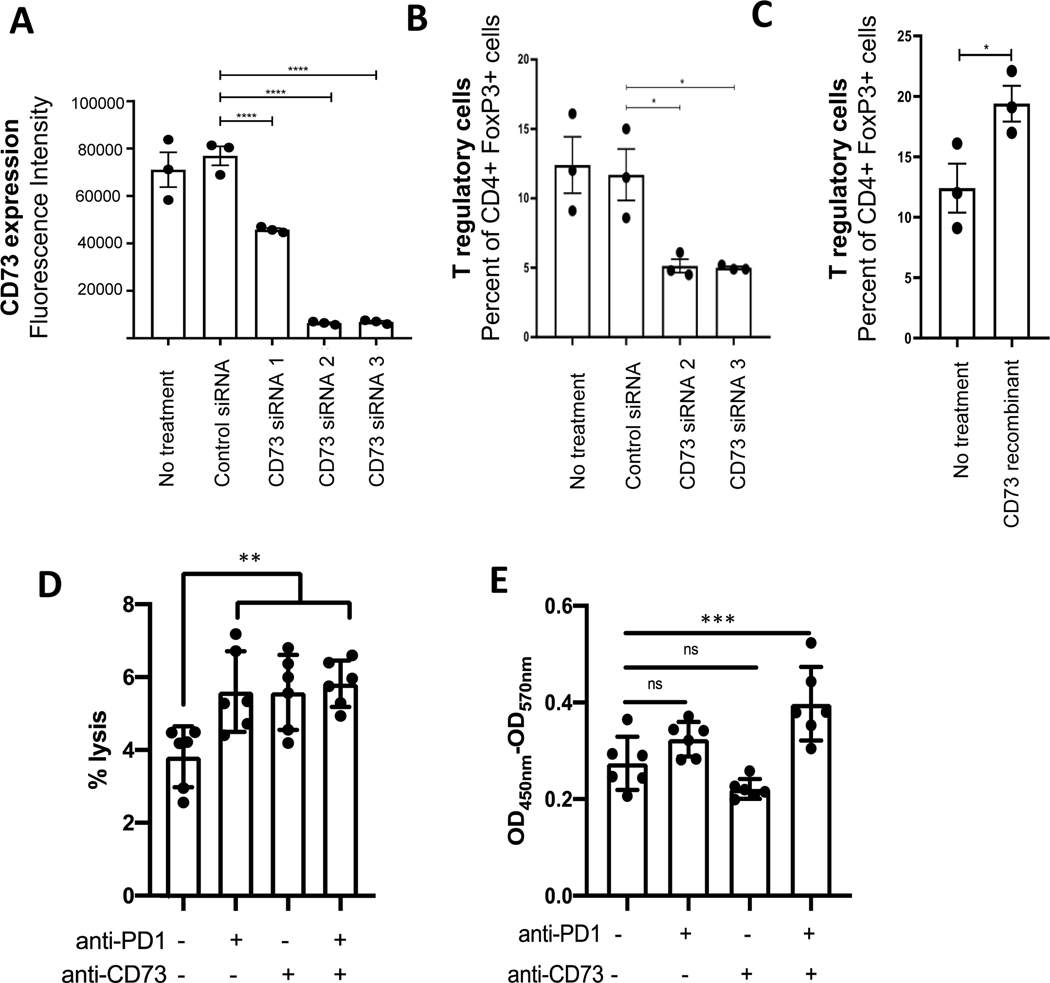
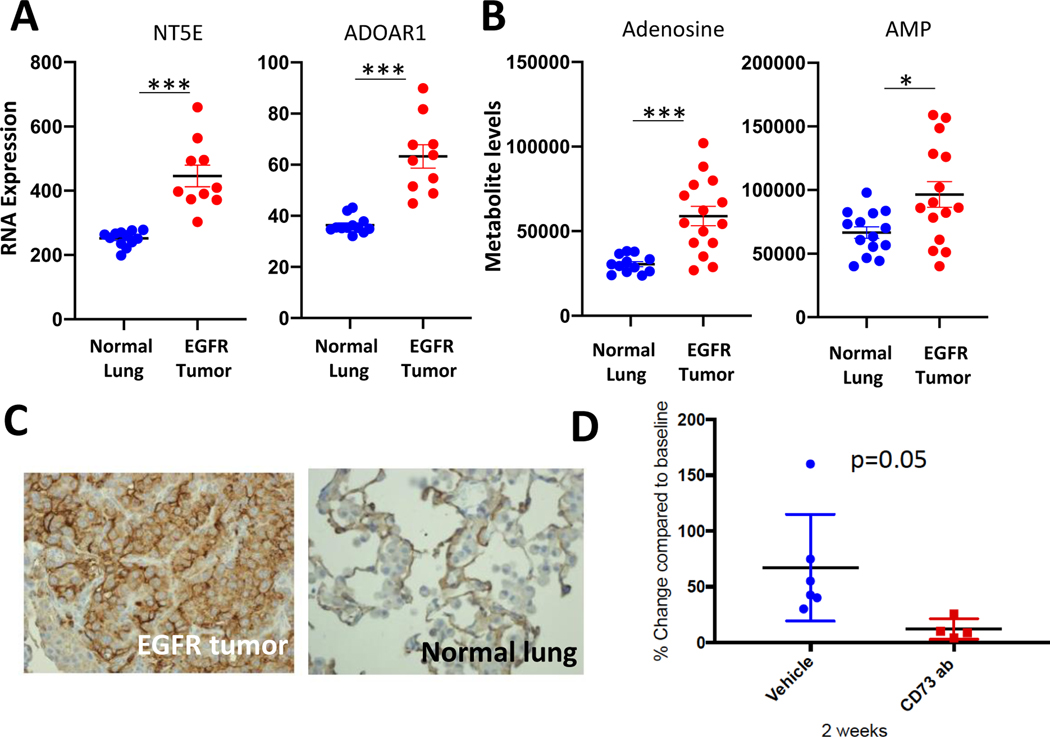
Results: EGFR-mutant NSCLC exhibited low programmed death-ligand 1, low tumor mutational burden, decreased number of cytotoxic T cells, and low T cell receptor clonality, consistent with an immune-inert phenotype, though T cell expansion ex vivo was preserved. In an analysis of 75 immune checkpoint genes, the top up-regulated genes in the EGFR-mutant tumors (NT5E and ADORA1) belonged to the CD73/adenosine pathway. Single-cell analysis revealed that the tumor cell population expressed CD73, both in the treatment-naive and resistant tumors. Using coculture systems with EGFR-mutant NSCLC cells, T regulatory cell proportion was decreased with CD73 knockdown. In an immune-competent mouse model of EGFR-mutant lung cancer, the CD73/adenosine pathway was markedly up-regulated and CD73 blockade significantly inhibited tumor growth.
Conclusions: Our work revealed that EGFR-mutant NSCLC has an immune-inert phenotype. We identified the CD73/adenosine pathway as a potential therapeutic target for EGFR-mutant NSCLC.
Keywords: Adenosine; CD73; EGFR-mutant lung cancer; Immune microenvironment; T cells.
Copyright © 2021 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Other authors do not report any relevant conflict of interest.
Figures
Comment in
-
CD73 and Adenosine Receptor Signaling as a Potential Therapeutic Target in EGFR-Mutated NSCLC.J Thorac Oncol. 2021 Apr;16(4):509-511. doi: 10.1016/j.jtho.2021.01.1623. J Thorac Oncol. 2021. PMID: 33781438 No abstract available.
-
Adenosine Pathway in NSCLC With Molecular Drivers: Can Oncogene Addiction Translate Into Immune Addiction?J Thorac Oncol. 2022 Mar;17(3):e35-e38. doi: 10.1016/j.jtho.2021.08.018. J Thorac Oncol. 2022. PMID: 35216738 No abstract available.
-
In Response.J Thorac Oncol. 2022 Mar;17(3):e39. doi: 10.1016/j.jtho.2022.01.003. J Thorac Oncol. 2022. PMID: 35216739 No abstract available.
References
-
- Lee CK, Man J, Lord S, Links M, Gebski V, Mok T, et al. Checkpoint Inhibitors in Metastatic EGFR-Mutated Non-Small Cell Lung Cancer-A Meta-Analysis. J Thorac Oncol. 2017;12(2):403–7. - PubMed
-
- Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fulop A, et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2016;375(19):1823–33. - PubMed
-
- Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015;372(21):2018–28. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
