

Remnant preservation provides good clinical outcomes after anterior cruciate ligament reconstruction
- PMID: 33388942
- PMCID: PMC8514348
- DOI: 10.1007/s00167-020-06406-6
Remnant preservation provides good clinical outcomes after anterior cruciate ligament reconstruction
Abstract
Purpose: To evaluate the association of remnant preservation (RP) and non-RP (NRP) with patient-reported outcome measures and subsequent graft rupture at a minimum 2-year follow-up after anterior cruciate ligament (ACL) reconstruction.
Methods: Patients in this retrospective study underwent primary isolated ACL reconstruction by the RP or NRP technique with a four- to five-strand hamstring tendon graft. Multivariate linear or logistic regression and Cox regression analyses were performed to compare the physical and psychological outcomes by the International Knee Documentation Committee subjective knee form (IKDC-SKF) and the Japanese Anterior Cruciate Ligament questionnaire 25 (JACL-25), respectively; satisfaction rate; and prognosticators of graft rupture.
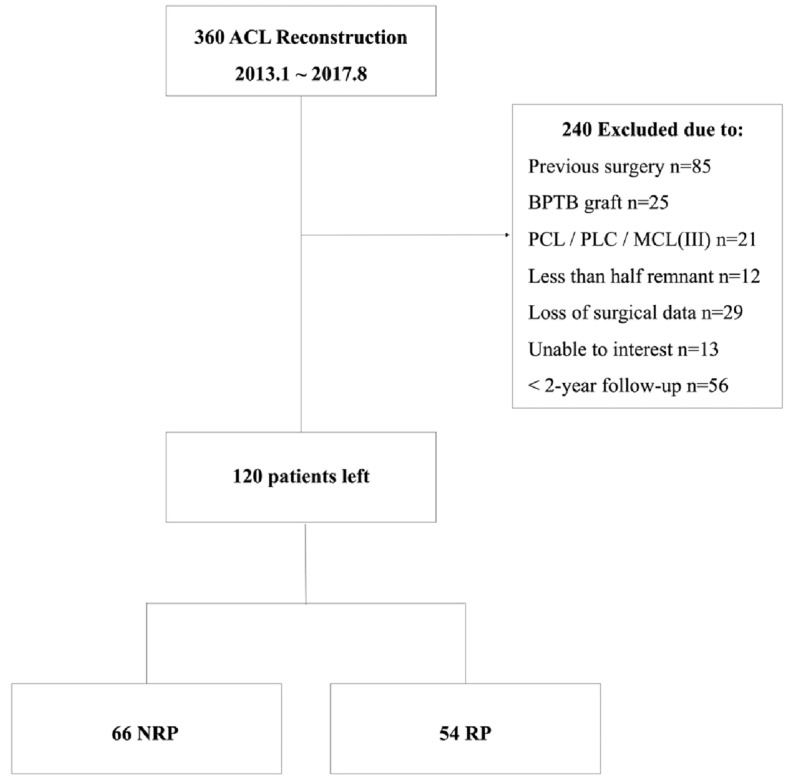
Results: In total, 120 patients (mean age, 30.6 ± 12.7 years; 54 RP, 66 NRP) with a mean follow-up of 3.2 ± 1.6 years were enrolled in this study. At the latest postoperative follow-up, the RP group showed a mean IKDC-SKF score of 92.3 ± 8.5 and mean JACL-25 score of 13.2 ± 11.2, while these scores in the NRP group were 86.4 ± 12.2 and 24.4 ± 19.5, respectively (P = 0.016 and 0.007, respectively). No significant differences were found in the return-to-sports rate (RP vs. NRP, 79.5% vs. 67.5%) or satisfaction rate (RP vs. NRP, 89.2% vs. 74.4%) (n.s.); however, a significant difference was found in the rate of return to the preinjury sports level (RP vs. NRP, 64.1% vs. 37.5%; P = 0.014). The graft rupture rate was significantly higher in the NRP than RP group (9/66 vs. 1/54; hazard ratio 9.29; 95% confidence interval 1.04-82.81). Younger age (≤ 18 years) was the other important risk factor for graft rupture (hazard ratio 8.67; 95% confidence interval 2.02-37.13).
Conclusion: Patients who underwent ACL reconstruction with the RP technique obtained somewhat better physical and psychological results than those who underwent ACL reconstruction with the NRP technique. With respect to clinical relevance, patients treated with the RP technique may obtain better outcomes in terms of graft rupture and return to the preinjury sports level than those treated with the NRP technique, but with no differences in overall return to sports or satisfaction.
Level of evidence: IV.
Keywords: Anterior cruciate ligament; Graft rupture; Psychological effects; Remnant preservation; Return to play.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
20-Year Outcomes of Anterior Cruciate Ligament Reconstruction With Hamstring Tendon Autograft: The Catastrophic Effect of Age and Posterior Tibial Slope.Am J Sports Med. 2018 Mar;46(3):531-543. doi: 10.1177/0363546517741497. Epub 2017 Dec 15. Am J Sports Med. 2018. PMID: 29244525
-
Anterolateral Ligament Reconstruction Is Associated With Significantly Reduced ACL Graft Rupture Rates at a Minimum Follow-up of 2 Years: A Prospective Comparative Study of 502 Patients From the SANTI Study Group.Am J Sports Med. 2017 Jun;45(7):1547-1557. doi: 10.1177/0363546516686057. Epub 2017 Feb 2. Am J Sports Med. 2017. PMID: 28151693
-
5-Year Survival of Pediatric Anterior Cruciate Ligament Reconstruction With Living Donor Hamstring Tendon Grafts.Am J Sports Med. 2019 Jan;47(1):41-51. doi: 10.1177/0363546518804502. Epub 2018 Nov 26. Am J Sports Med. 2019. PMID: 30476437
-
Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Outcomes for Quadriceps Tendon Autograft Versus Bone-Patellar Tendon-Bone and Hamstring-Tendon Autografts.Am J Sports Med. 2019 Dec;47(14):3531-3540. doi: 10.1177/0363546518825340. Epub 2019 Feb 21. Am J Sports Med. 2019. PMID: 30790526
-
A meta-analysis of bone-patellar tendon-bone autograft versus four-strand hamstring tendon autograft for anterior cruciate ligament reconstruction.Knee. 2015 Mar;22(2):100-10. doi: 10.1016/j.knee.2014.11.014. Epub 2014 Dec 11. Knee. 2015. PMID: 25547048 Review.
Cited by
-
The effects of remnant-preserving anterior cruciate ligament reconstruction on proprioception: A prospective comparative study.Acta Orthop Traumatol Turc. 2023 May;57(3):109-115. doi: 10.5152/j.aott.2023.21365. Acta Orthop Traumatol Turc. 2023. PMID: 37395355 Free PMC article.
-
Anterior Cruciate Ligament Hybrid Remnant Preservation Reconstruction Demonstrates Equivalent Patient-Reported Outcomes and Complications as Traditional Anterior Cruciate Ligament Reconstruction After 1 Year.Arthrosc Sports Med Rehabil. 2024 Feb 1;6(2):100875. doi: 10.1016/j.asmr.2023.100875. eCollection 2024 Apr. Arthrosc Sports Med Rehabil. 2024. PMID: 38328529 Free PMC article.
-
The posterior cruciate ligament index as a reliable indirect sign of anterior cruciate ligament rupture is associated with the course of knee joint injury.Knee Surg Sports Traumatol Arthrosc. 2023 Aug;31(8):3277-3283. doi: 10.1007/s00167-023-07357-4. Epub 2023 Mar 11. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36899193
-
Good clinical and radiological results following remnant-preserving posterior cruciate ligament reconstruction: a systematic review.Knee Surg Sports Traumatol Arthrosc. 2023 Jun;31(6):2418-2432. doi: 10.1007/s00167-022-07192-z. Epub 2022 Oct 8. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36208342 Free PMC article.
-
Anatomical Inside-Out Remnant-Preserving Anterior Cruciate Ligament Reconstruction: A Surgical Technique for Biological Anterior Cruciate Ligament Reconstruction.Arthrosc Tech. 2025 Mar 3;14(6):103503. doi: 10.1016/j.eats.2025.103503. eCollection 2025 Jun. Arthrosc Tech. 2025. PMID: 40656743 Free PMC article.
References
-
- Demirag B, Ermutlu C, Aydemir F, Durak K. A comparison of clinical outcome of augmentation and standard reconstruction techniques for partial anterior cruciate ligament tears. Eklem Hast Cerrahisi. 2012;23:140–144. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
