

Systematic volumetric analysis predicts response to CSF drainage and outcome to shunt surgery in idiopathic normal pressure hydrocephalus
- PMID: 33389035
- PMCID: PMC8213563
- DOI: 10.1007/s00330-020-07531-z
Systematic volumetric analysis predicts response to CSF drainage and outcome to shunt surgery in idiopathic normal pressure hydrocephalus
Abstract
Objectives: Idiopathic normal pressure hydrocephalus (INPH) is a neurodegenerative disorder characterized by excess cerebrospinal fluid (CSF) in the ventricles, which can be diagnosed by invasive CSF drainage test and treated by shunt placement. Here, we aim to investigate the diagnostic and prognostic power of systematic volumetric analysis based on brain structural MRI for INPH.
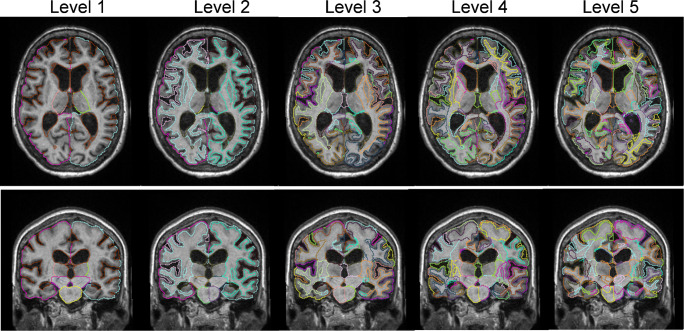
Methods: We performed a retrospective study with a cohort of 104 probable INPH patients who underwent CSF drainage tests and another cohort of 41 INPH patients who had shunt placement. High-resolution T1-weighted images of the patients were segmented using an automated pipeline into 283 structures that are grouped into different granularity levels for volumetric analysis. Volumes at multi-granularity levels were used in a recursive feature elimination model to classify CSF drainage responders and non-responders. We then used pre-surgical brain volumes to predict Tinetti and MMSE scores after shunting, based on the least absolute shrinkage and selection operator.
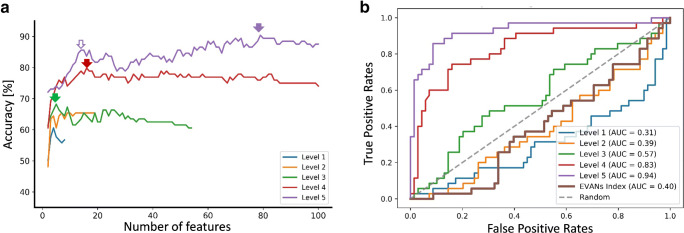
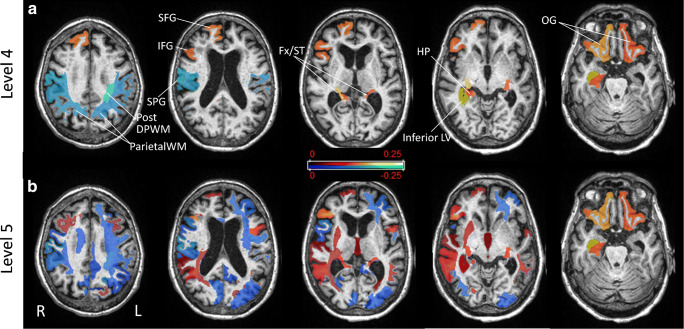
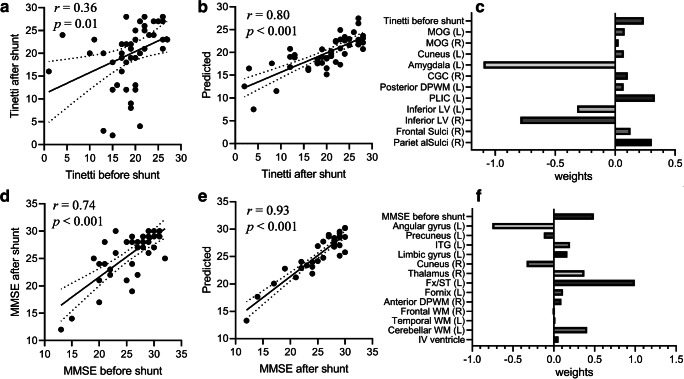
Results: The classification accuracy of differentiating the CSF drainage responders and non-responders increased as the granularity increased. The highest diagnostic accuracy was achieved at the finest segmentation with a sensitivity/specificity/precision/accuracy of 0.89/0.91/0.84/0.90 and an area under the curve of 0.94. The predicted post-surgical neurological scores showed high correlations with the ground truth, with r = 0.80 for Tinetti and r = 0.88 for MMSE. The anatomical features that played important roles in the diagnostic and prognostic tasks were also illustrated.
Conclusions: We demonstrated that volumetric analysis with fine segmentation could reliably differentiate CSF drainage responders from other INPH-like patients, and it could accurately predict the neurological outcomes after shunting.
Key points: • We performed a fully automated segmentation of brain MRI at multiple granularity levels for systematic volumetric analysis of idiopathic normal pressure hydrocephalus (INPH) patients. • We were able to differentiate patients that responded to CSF drainage test with an accuracy of 0.90 and area under the curve of 0.94 in a cohort of 104 probable INPH patients, as well as to predict the post-shunt gait and cognitive scores with a coefficient of 0.80 for Tinetti and 0.88 for MMSE. • Feature analysis showed the inferior lateral ventricle, bilateral hippocampus, and orbital cortex are positive indicators of CSF drainage responders, whereas the posterior deep white matter and parietal subcortical white matter were negative predictors.
Keywords: Algorithm; Hydrocephalus; Normal pressure; Segmentation; Volume.
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies: Dr. Susumu Mori is associated with AnatomyWorks LLC.
Figures
Similar articles
-
Use of cortical volume to predict response to temporary CSF drainage in patients with idiopathic normal pressure hydrocephalus.J Neurosurg. 2023 May 5;139(6):1776-1783. doi: 10.3171/2023.3.JNS222787. Print 2023 Dec 1. J Neurosurg. 2023. PMID: 37148227
-
The role of diffusion tensor imaging and fractional anisotropy in the evaluation of patients with idiopathic normal pressure hydrocephalus: a literature review.Neurosurg Focus. 2016 Sep;41(3):E12. doi: 10.3171/2016.6.FOCUS16192. Neurosurg Focus. 2016. PMID: 27581308 Review.
-
Evaluating the cerebrospinal fluid tap test with the Hellström iNPH scale for patients with idiopathic normal pressure hydrocephalus.Fluids Barriers CNS. 2021 Apr 7;18(1):18. doi: 10.1186/s12987-021-00252-5. Fluids Barriers CNS. 2021. PMID: 33827613 Free PMC article.
-
Diagnosis, treatment, and analysis of long-term outcomes in idiopathic normal-pressure hydrocephalus.Neurosurgery. 2005 Oct;57(4):699-705; discussion 699-705. doi: 10.1093/neurosurgery/57.4.699. Neurosurgery. 2005. PMID: 16239882
-
Radiological predictors of shunt response in the diagnosis and treatment of idiopathic normal pressure hydrocephalus: a systematic review and meta-analysis.Acta Neurochir (Wien). 2023 Feb;165(2):369-419. doi: 10.1007/s00701-022-05402-8. Epub 2022 Nov 26. Acta Neurochir (Wien). 2023. PMID: 36435931 Free PMC article.
Cited by
-
Inadequacies in iNPH diagnosis: envisioning a paradigm shift towards integrated, multi-modal testing, and consensus-driven research for improved patient outcomes.Acta Neurochir (Wien). 2023 Dec;165(12):4055-4058. doi: 10.1007/s00701-023-05754-9. Epub 2023 Aug 14. Acta Neurochir (Wien). 2023. PMID: 37578505 No abstract available.
-
Predicting Gait Speed Improvement in Idiopathic Normal Pressure Hydrocephalus Patients: The Role of Evans Index and Ventricular Volume.Cureus. 2024 Jun 6;16(6):e61799. doi: 10.7759/cureus.61799. eCollection 2024 Jun. Cureus. 2024. PMID: 38975434 Free PMC article.
-
Predictors of Satisfactory Surgical Outcome in Idiopathic Normal Pressure Hydrocephalus (Review).Sovrem Tekhnologii Med. 2024;16(2):68-77. doi: 10.17691/stm2024.16.2.07. Epub 2024 Apr 27. Sovrem Tekhnologii Med. 2024. PMID: 39539751 Free PMC article.
-
The Role of Machine Learning and Radiomics for Treatment Response Prediction in Idiopathic Normal Pressure Hydrocephalus.Cureus. 2021 Oct 5;13(10):e18497. doi: 10.7759/cureus.18497. eCollection 2021 Oct. Cureus. 2021. PMID: 34754658 Free PMC article.
-
The Diagnostic Accuracy of Artificial Intelligence in Radiological Markers of Normal-Pressure Hydrocephalus (NPH) on Non-Contrast CT Scans of the Brain.Diagnostics (Basel). 2023 Sep 1;13(17):2840. doi: 10.3390/diagnostics13172840. Diagnostics (Basel). 2023. PMID: 37685378 Free PMC article.
References
-
- Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PM (2005) Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery 57:S4–S16 discussion ii-v - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
