

The Current Landscape of Antibody-based Therapies in Solid Malignancies
- PMID: 33391547
- PMCID: PMC7738893
- DOI: 10.7150/thno.52614
The Current Landscape of Antibody-based Therapies in Solid Malignancies
Abstract
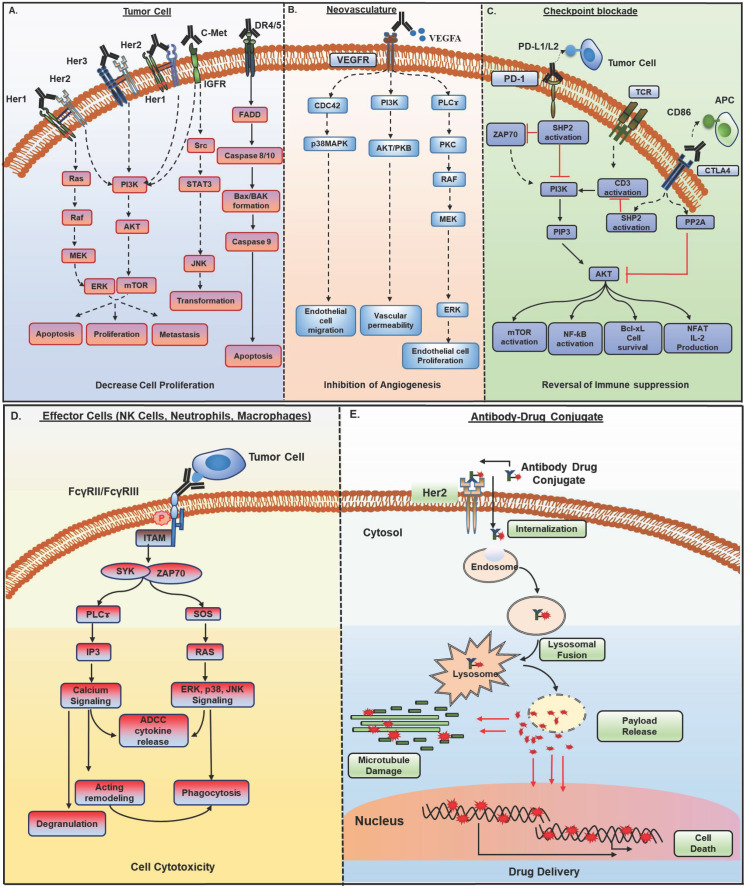
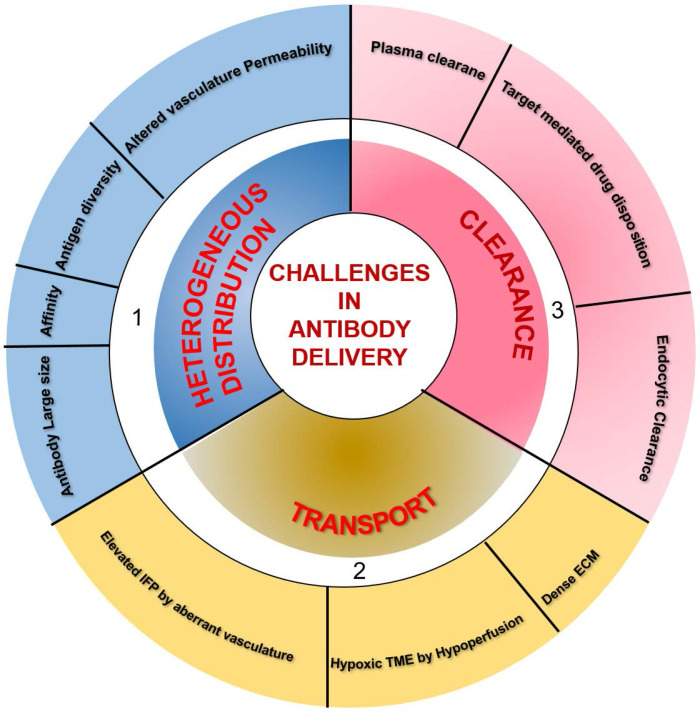
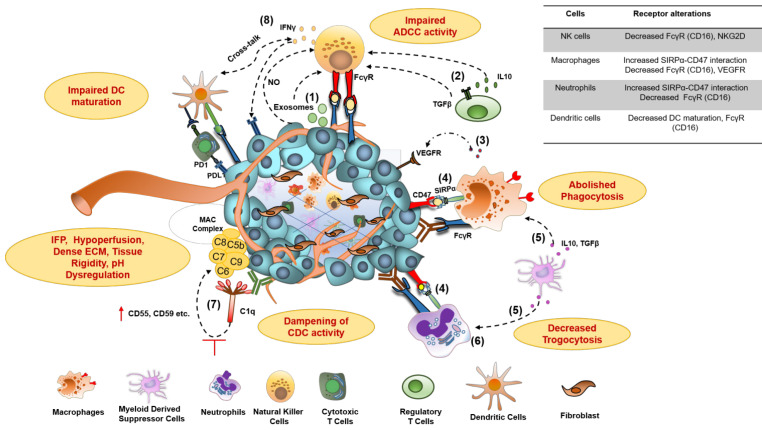
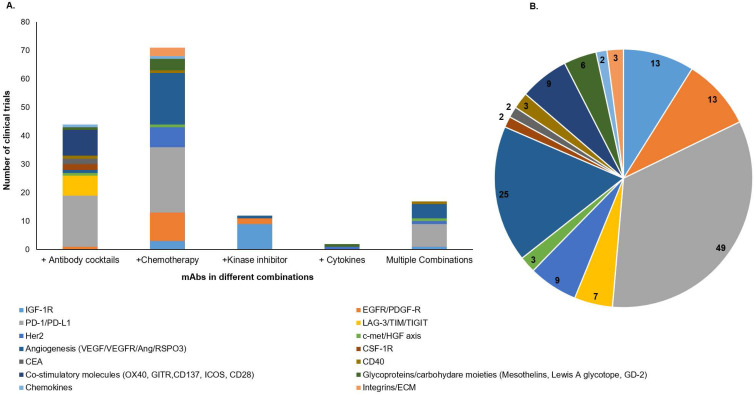
Over the past three decades, monoclonal antibodies (mAbs) have revolutionized the landscape of cancer therapy. Still, this benefit remains restricted to a small proportion of patients due to moderate response rates and resistance emergence. The field has started to embrace better mAb-based formats with advancements in molecular and protein engineering technologies. The development of a therapeutic mAb with long-lasting clinical impact demands a prodigious understanding of target antigen, effective mechanism of action, gene engineering technologies, complex interplay between tumor and host immune system, and biomarkers for prediction of clinical response. This review discusses the various approaches used by mAbs for tumor targeting and mechanisms of therapeutic resistance that is not only caused by the heterogeneity of tumor antigen, but also the resistance imposed by tumor microenvironment (TME), including inefficient delivery to the tumor, alteration of effector functions in the TME, and Fc-gamma receptor expression diversity and polymorphism. Further, this article provides a perspective on potential strategies to overcome these barriers and how diagnostic and prognostic biomarkers are being used in predicting response to mAb-based therapies. Overall, understanding these interdependent parameters can improve the current mAb-based formulations and develop novel mAb-based therapeutics for achieving durable clinical outcomes in a large subset of patients.
Keywords: Antibodies; cancer; challenges; mechanisms of action; therapy.
© The author(s).
Conflict of interest statement
Competing Interests: SKB is one of the co-founders of Sanguine Diagnostics and Therapeutics, Inc. The other authors disclosed no potential conflicts of interest.
Figures
References
-
- Sulek K. [Prize in 1908 awarded to P. Ehrlich and E. Metchnikoff for their work in immunology] Wiad Lek. 1967;20:1117–8. - PubMed
-
- Carter PJ, Lazar GA. Next generation antibody drugs: pursuit of the 'high-hanging fruit'. Nat Rev Drug Discov. 2018;17:197–223. - PubMed
-
- London M, Gallo E. Epidermal growth factor receptor (EGFR) involvement in epithelial-derived cancers and its current antibody-based immunotherapies. Cell Biol Int. 2020;44:1267–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
