

Association between anterior talofibular ligament injury and ankle tendon, ligament, and joint conditions revealed by magnetic resonance imaging
- PMID: 33392013
- PMCID: PMC7719946
- DOI: 10.21037/qims-20-5
Association between anterior talofibular ligament injury and ankle tendon, ligament, and joint conditions revealed by magnetic resonance imaging
Abstract
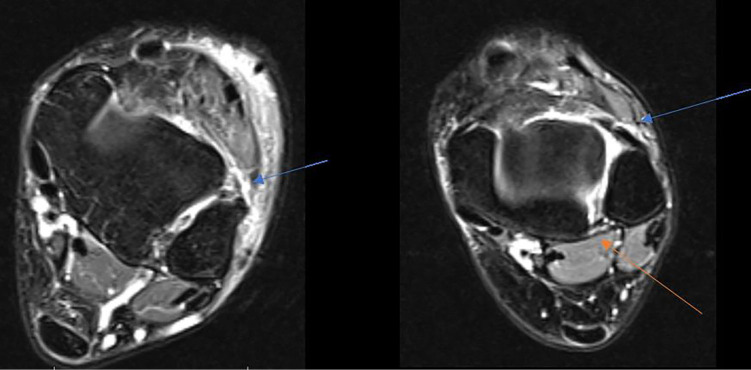
Background: The lateral ankle ligament complex is the most frequently injured ligament secondary to strong ankle inversion movement during lateral ankle sprains (LAS). Among these injuries, anterior talofibular ligament (ATFL) injury is the most frequent condition (present in 66-85% of such injuries). The purpose of this research was to use magnetic resonance imaging (MRI) to determine the association between ankle tendon, ligament, and joint conditions and ATFL injuries.
Methods: A case-control MRI study was carried out to compare the presence of ankle muscle, tendon, ligament, and joint conditions in patients with injured ATFLs (case group; n=25) and non-injured ATFLs (control group; n=25).
Results: Achilles tendinopathy was present in 1/25 (4%) patients with injured ATFLs and 7/25 (28%) non-injured ATFL subjects (P=0.048). Injured calcaneofibular ligaments (CFLs) were present in 19/25 (76%) patients with injured ATFLs and 1/25 (4%) non-injured ATFL subjects (P<0.001). Finally, injured tibiotalar joints were present in 16/25 (64%) patients with injured ATFLs and 5/25 (20%) non-injured ATFL subjects (P=0.002). Other musculoskeletal structure injuries occurred at similar rates between patients with injured ATFLs and those with non-injured ATLFs (P≥0.05).
Conclusions: Patients with ATFL injuries showed a greater presence of CFL and tibiotalar joint injuries than subjects with non-injured ATFLs.
Keywords: Ankle injuries; magnetic resonance imaging (MRI); musculoskeletal diseases; sprains and strains.
2021 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/qims-20-5). The authors have no conflicts of interest to declare.
Figures









References
LinkOut - more resources
Full Text Sources
Other Literature Sources