

Iron and Chronic Kidney Disease: Still a Challenge
- PMID: 33392212
- PMCID: PMC7775475
- DOI: 10.3389/fmed.2020.565135
Iron and Chronic Kidney Disease: Still a Challenge
Abstract
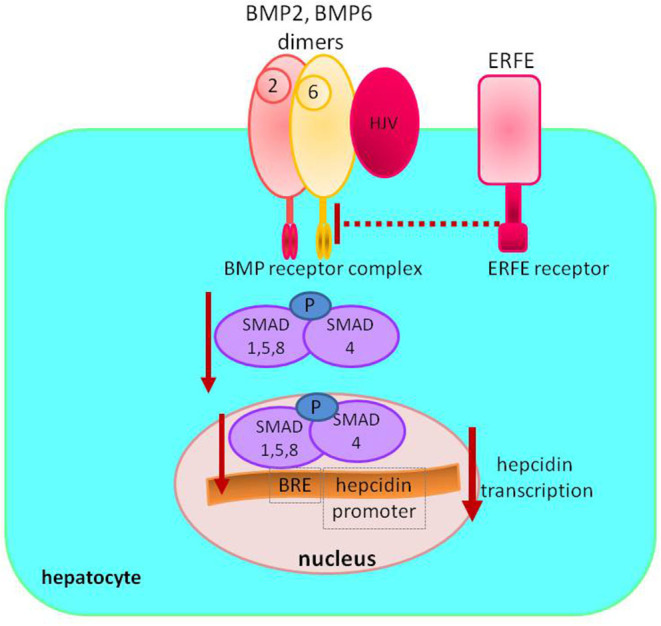
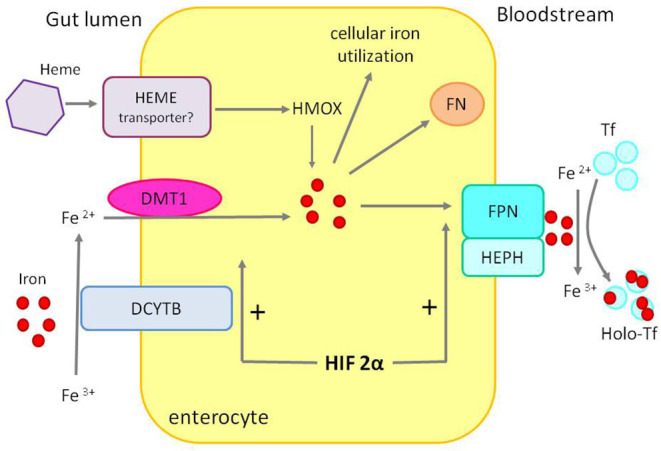
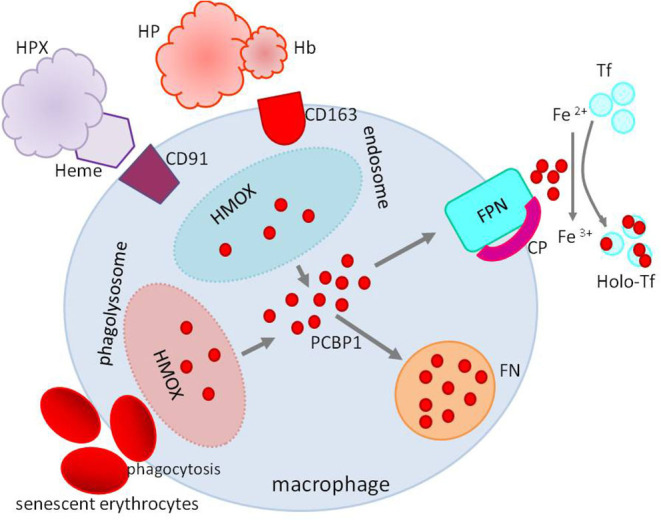
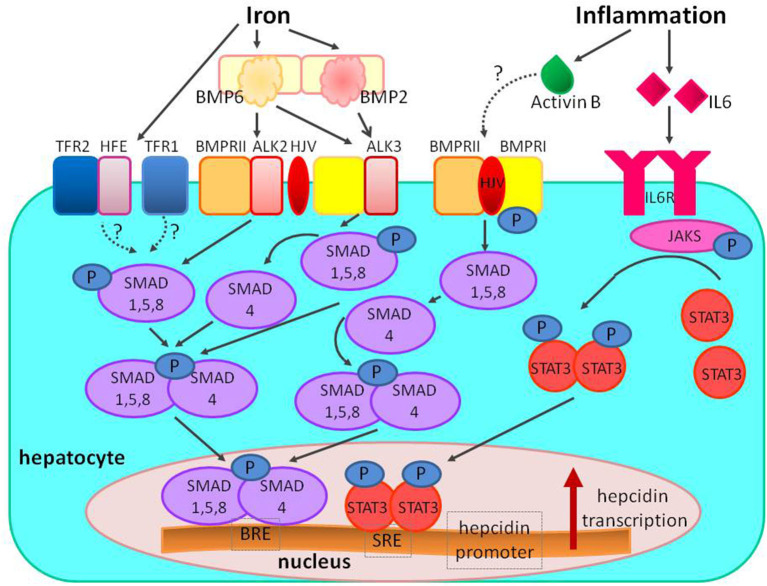
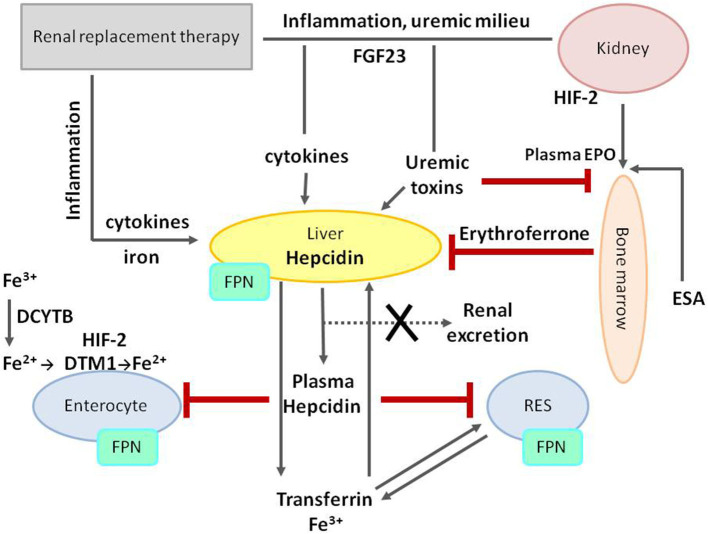
Anemia is a clinical feature of chronic kidney disease (CKD). Most common causes are iron and erythropoietin deficiency. The last two decades have yielded significant advances in understanding iron balance's physiology, including iron trafficking and the crosstalk between iron, oxygen, and erythropoiesis. This knowledge sheds new light on the regulation and disturbance of iron homeostasis in CKD and holds the promise for developing new diagnostic and therapeutic tools to improve the management of iron disorders. Hepcidin-ferroportin axis has a central role in regulating body iron balance and coordinating communication between tissues and cells that acquire, store, and utilize iron. Recent research has revealed a bidirectional relationship between fibroblast growth factor 23 (FGF23) and iron status, anemia, and inflammation, as well as the role of erythroferrone (ERFE) in iron homeostasis. However, ERFE concentrations and actions are not well-characterized in CKD patients. Studies on ERFE in CKD are limited with slightly conflicting results. Despite general interest in iron metabolism in kidney diseases, studies on the less prevalent renal replacement therapy mode, such as peritoneal dialysis or hemodiafiltration, are scarce. Slightly more was published on hemodialysis. There are several novel options on the horizon; however, clinical data are limited. One should be aware of the potential risks and benefits of the novel, sophisticated therapies. An inhibition of hepcidin on the different pathways might be also a viable adjunctive therapeutic option in other clinical situations.
Keywords: HIF-1α; anemia; chronic kidney disease; erythroferrone; hepcidin; iron.
Copyright © 2020 Wojtaszek, Glogowski and Malyszko.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Wong MMY, Tu C, Li Y, Perlman RL, Pecotis-Filho R, Lopes AA, et al. . Anemia and iron deficiency among chronic kidney disease Stages 3-5ND patients in the Chronic Kidney Disease Outcomes and Practice Patterns Study: often unmeasured, variably treated. Clin Kiney J. (2019) 13:613–24. 10.1093/ckj/sfz091 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical