

Delayed diagnosis of prosopagnosia following a hemorrhagic stroke in an elderly man: A case report
- PMID: 33392335
- PMCID: PMC7760442
- DOI: 10.12998/wjcc.v8.i24.6487
Delayed diagnosis of prosopagnosia following a hemorrhagic stroke in an elderly man: A case report
Abstract
Background: Acquired prosopagnosia is a rare condition characterized by the loss of familiarity with previously known faces and the inability to recognize new ones. It usually occurs after the onset of brain lesions such as in a stroke. The initial identification of prosopagnosia generally relies on a patient's self-report, which can be challenging if it lacks an associated chief complaint. There were few cases of prosopagnosia presenting purely as eye symptoms in the previous literature confirmed by functional magnetic resonance imaging (MRI).
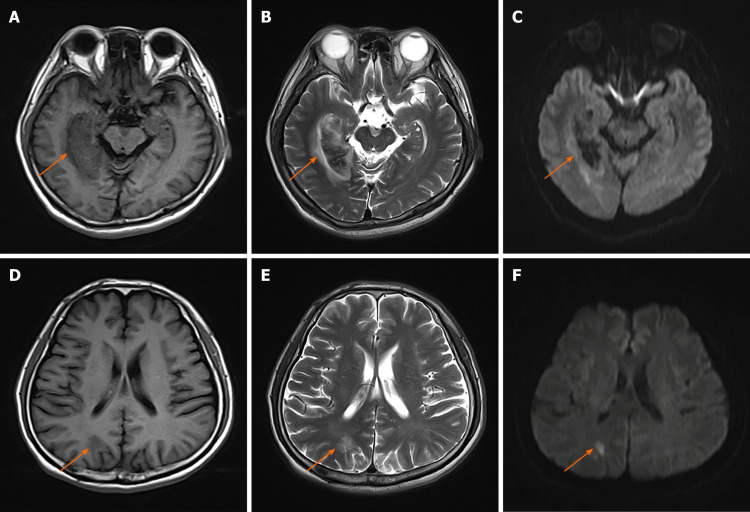
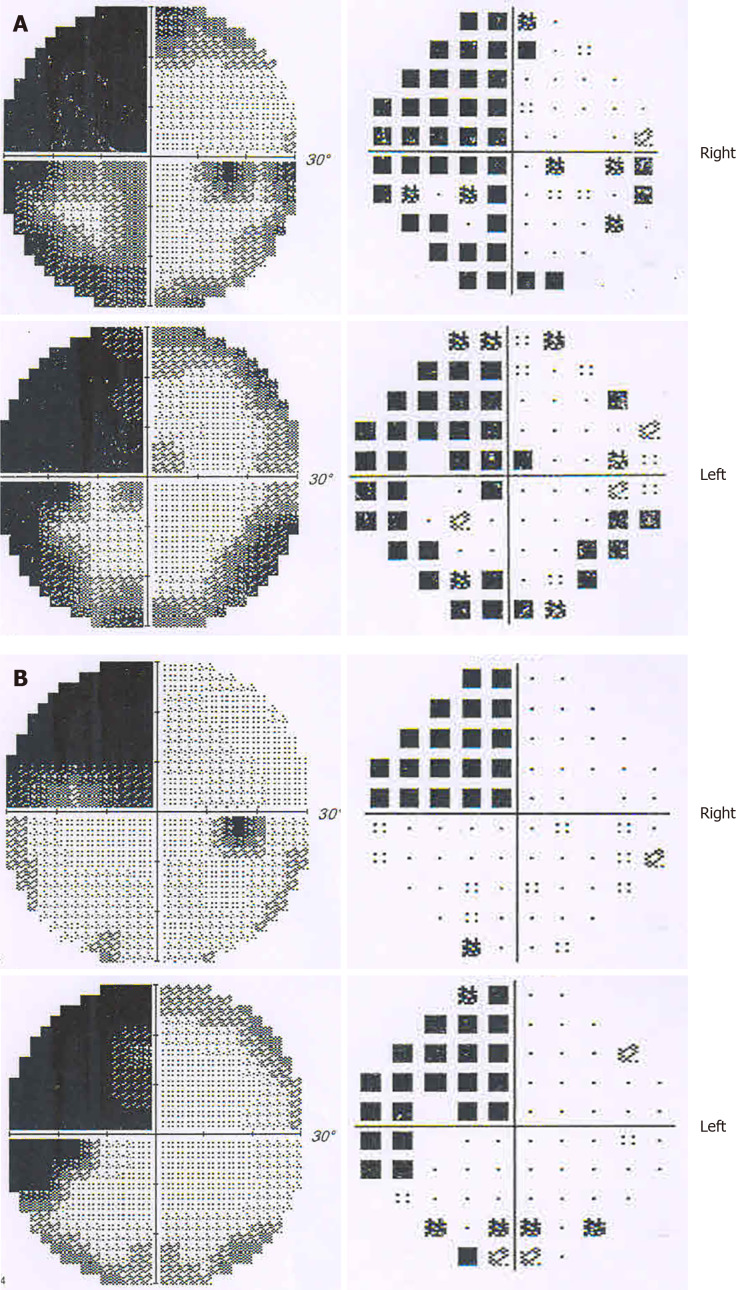
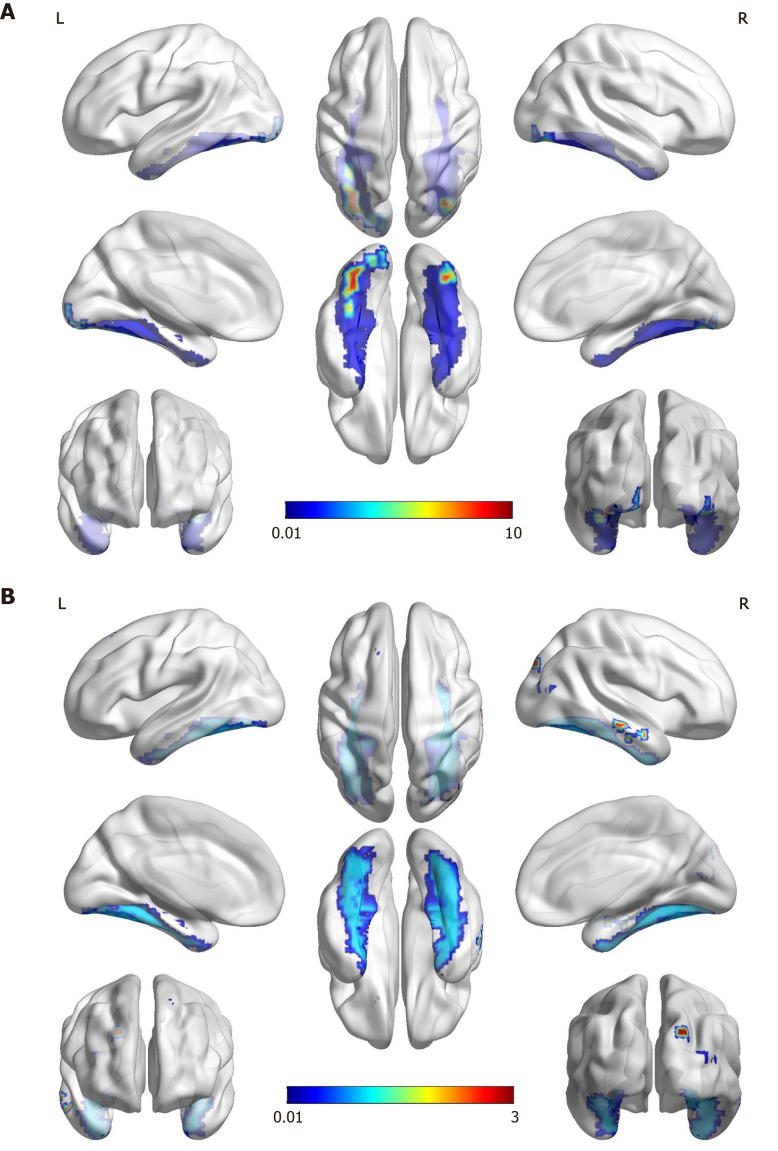
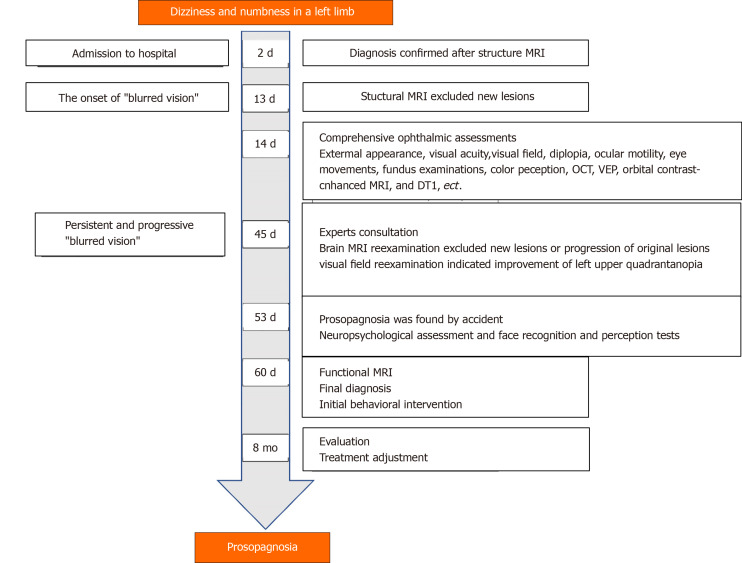
Case summary: We present a case of delayed diagnosis of prosopagnosia after a right hemisphere stroke in an elderly man whose chief complaint was persistent and progressive "blurred vision" without facial recognition impairment. Ophthalmic tests revealed a homonymous left upper quadrantanopia, with normal visual acuity. He was found by accident to barely recognize familiar faces. The patient showed severe deficit in face recognition and perception tests, and mild memory loss in neuropsychological assessments. Further functional MRI revealed the visual recognition deficits were face-specific. After behavioral intervention, the patient started to rely on other cues to compensate for poor facial recognition. His prosopagnosia showed no obvious improvement eight months after the stroke, which had negative impact on his social network.
Conclusion: Our case demonstrates that the presentation of prosopagnosia can be atypical, and visual difficulties might be a clinical manifestation solely of prosopagnosia, which emphasizes the importance of routinely considering face recognition impairment among elderly patients with brain lesions.
Keywords: Blurred vision; Case report; Diagnosis; Elderly; Functional magnetic resonance imaging; Prosopagnosia; Stroke.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Right Fusiform Gyrus Infarct with Acute Prosopagnosia.Acta Neurol Taiwan. 2022 Dec 30;31(4):186-187. Acta Neurol Taiwan. 2022. PMID: 35470413
-
[False recognition of faces associated with fronto-temporal dementia with prosopagnosia].Rev Neurol (Paris). 2005 Sep;161(8-9):804-16. doi: 10.1016/s0035-3787(05)85139-2. Rev Neurol (Paris). 2005. PMID: 16244562 French.
-
Understanding the functional neuroanatomy of acquired prosopagnosia.Neuroimage. 2007 Apr 1;35(2):836-52. doi: 10.1016/j.neuroimage.2006.09.051. Epub 2007 Feb 14. Neuroimage. 2007. PMID: 17303440
-
[Non-verbal facial and topographic visual object agnosia--a problem of familiarity in prosopagnosia and topographic disorientation].No To Shinkei. 1989 Jul;41(7):703-10. No To Shinkei. 1989. PMID: 2684250 Review. Japanese.
-
Prosopagnosia after stroke: potentials for impairment and treatment.Top Stroke Rehabil. 2013 Nov-Dec;20(6):471-7. doi: 10.1310/tsr2006-471. Top Stroke Rehabil. 2013. PMID: 24273293 Review.
Cited by
-
An analysis of patients with a chief complaint of difficulty moving.J Rural Med. 2023 Jan;18(1):36-41. doi: 10.2185/jrm.2022-016. Epub 2023 Jan 6. J Rural Med. 2023. PMID: 36700130 Free PMC article.
-
Treatment of transient prosopagnosia with a tyrosine kinase inhibitor in a case of brain metastasis from EGFR-mutated lung adenocarcinoma.Surg Neurol Int. 2022 Jul 1;13:280. doi: 10.25259/SNI_500_2022. eCollection 2022. Surg Neurol Int. 2022. PMID: 35855154 Free PMC article.
References
-
- Davies-Thompson J, Pancaroglu R, Barton J. Acquired prosopagnosia: structural basis and processing impairments. Front Biosci (Elite Ed) 2014;6:159–174. - PubMed
-
- Schmidt D. Neuro-ophthalmological findings in patients with acquired prosopagnosia. Graefes Arch Clin Exp Ophthalmol. 2015;253:333–334. - PubMed
-
- Fadelalla M, Kanodia A, Elsheikh M, Ellis J, Smith V, Hossain-Ibrahim K. A case of aneurysmal subarchnoid haemorrhage and superficial siderosis complicated by prospagnosia, simultagnosia and alexia without agraphia. Br J Neurosurg. 2019:1–4. - PubMed
-
- Monti C, Sozzi M, Bossi F, Corbo M, Rivolta D. Atypical holistic processing of facial identity and expression in a case of acquired prosopagnosia. Cogn Neuropsychol. 2019;36:358–382. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
