

Trends and Geographic Variation in Acute Respiratory Failure and ARDS Mortality in the United States
- PMID: 33393472
- PMCID: PMC7581392
- DOI: 10.1016/j.chest.2020.10.042
Trends and Geographic Variation in Acute Respiratory Failure and ARDS Mortality in the United States
Abstract
Background: Despite numerous advances in the understanding of the pathophysiology, progression, and management of acute respiratory failure (ARF) and ARDS, limited contemporary data are available on the mortality burden of ARF and ARDS in the United States.
Research question: What are the contemporary trends and geographic variation in ARF and ARDS-related mortality in the United States?
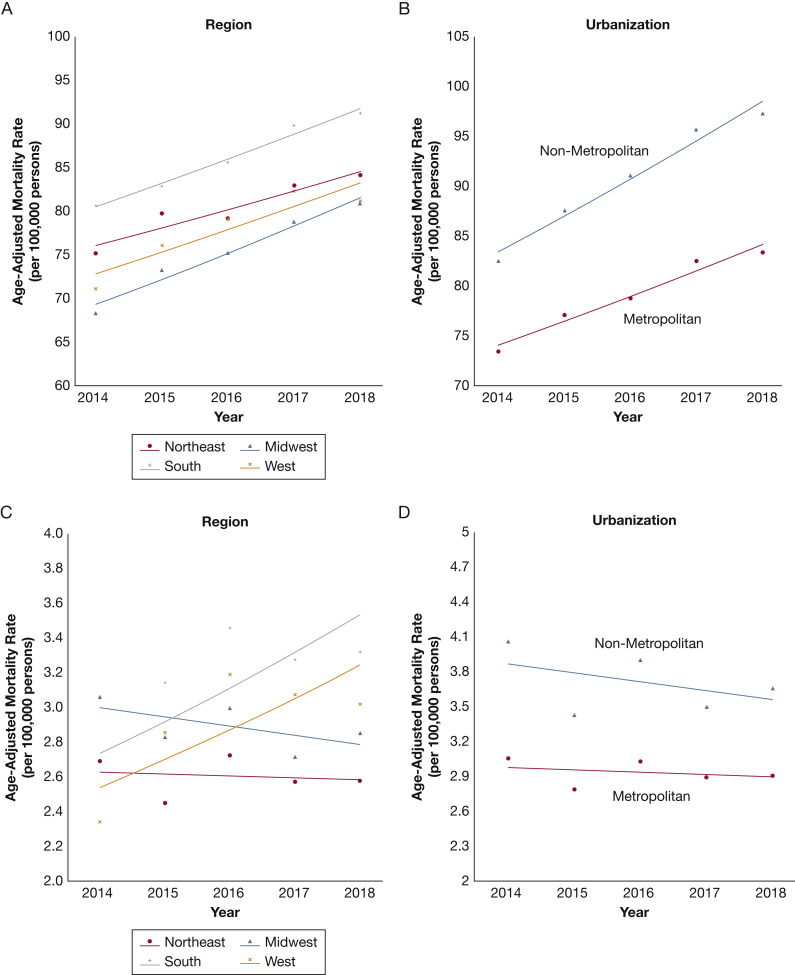
Study design and methods: A retrospective analysis of the National Center for Health Statistics' nationwide mortality data was conducted to assess the ARF and ARDS-related mortality trends from 2014 through 2018 and the geographic distribution of ARF and ARDS-related deaths in 2018 for all American residents. Piecewise linear regression was used to evaluate the trends in age-adjusted mortality rates (AAMRs) in the overall population and various demographic subgroups of age, sex, race, urbanization, and region.
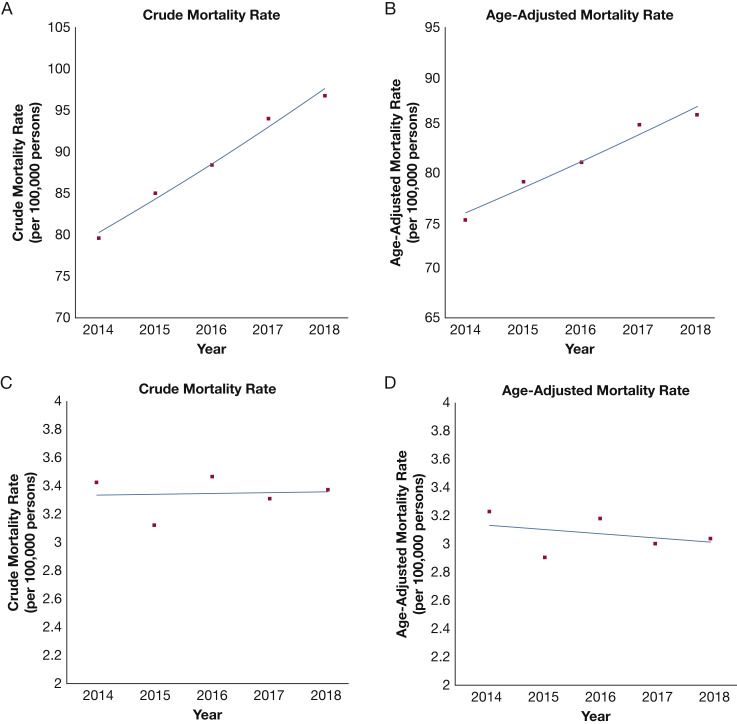
Results: Among 1,434,349 ARF-related deaths and 52,958 ARDS-related deaths during the study period, the AAMR was highest in older individuals (≥ 65 years), non-Hispanic Black people, and those living in the nonmetropolitan region. The AAMR for ARF-related deaths (per 100,000 people) increased from 74.9 (95% CI, 74.6-75.2) in 2014 to 85.6 (95% CI, 85.3-85.9) in 2018 (annual percentage change [APC], 3.4 [95% CI, 2.2-4.6]; Ptrend = .003). The AAMR (per 100,000 people) for ARDS-related deaths was 3.2 (95% CI, 3.2-3.3) in 2014 and 3.0 (95% CI, 3.0-3.1 in 2018; APC, -0.9 [95% CI, -5.4 to 3.8]; Ptrend = .56). The observed increase in rates for ARF mortality was consistent across the subgroups of age, sex, race or ethnicity, urbanization status, and geographical region (Ptrend < .05 for all). The AAMR (per 100,000 people) for ARF (91.3 [95% CI, 90.8-91.8]) and ARDS-related mortality (3.3 [95% CI, 3.2-3.4]) in 2018 were highest in the South.
Interpretation: The ARF-related mortality increased at approximately 3.4% annually, and ARDS-related mortality showed a lack of decline in the last 5 years. These data contextualize important health information to guide priorities for research, clinical care, and policy, especially during the coronavirus disease 2019 pandemic in the United States.
Keywords: ARDS; coronavirus disease; mortality; risk factors.
Copyright © 2020 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Bellani G., Laffey J.G., Pham T., et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. - PubMed
-
- Pham T., Rubenfeld G.D. Fifty years of research in ARDS. The epidemiology of acute respiratory distress syndrome. A 50th birthday review. Am J Respir Crit Care Med. 2017;195(7):860–870. - PubMed
-
- Fan E., Brodie D., Slutsky A.S. Acute respiratory distress syndrome: advances in diagnosis and treatment. JAMA. 2018;319(7):698–710. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
