

Identifying the Distinct Cognitive Phenotypes in Multiple Sclerosis
- PMID: 33393981
- PMCID: PMC7783596
- DOI: 10.1001/jamaneurol.2020.4920
Identifying the Distinct Cognitive Phenotypes in Multiple Sclerosis
Abstract
Importance: Cognitive impairment is a common and disabling feature of multiple sclerosis (MS), but a precise characterization of cognitive phenotypes in patients with MS is lacking.
Objectives: To identify cognitive phenotypes in a clinical cohort of patients with MS and to characterize their clinical and magnetic resonance imaging (MRI) features.
Design, setting, and participants: This multicenter cross-sectional study consecutively screened clinically stable patients with MS and healthy control individuals at 8 MS centers in Italy from January 1, 2010, to October 31, 2019. Patients with MS and healthy control individuals who were not using psychoactive drugs and had no history of other neurological or medical disorders, learning disability, severe head trauma, and alcohol or drug abuse were enrolled.
Main outcomes and measures: Participants underwent a neurological examination and a cognitive evaluation with the Rao Brief Repeatable Battery and Stroop Color and Word Test. A subgroup of participants also underwent a brain MRI examination. Latent profile analysis was used on cognitive test z scores to identify cognitive phenotypes. Linear regression and mixed-effects models were used to define clinical and MRI features of each phenotype.
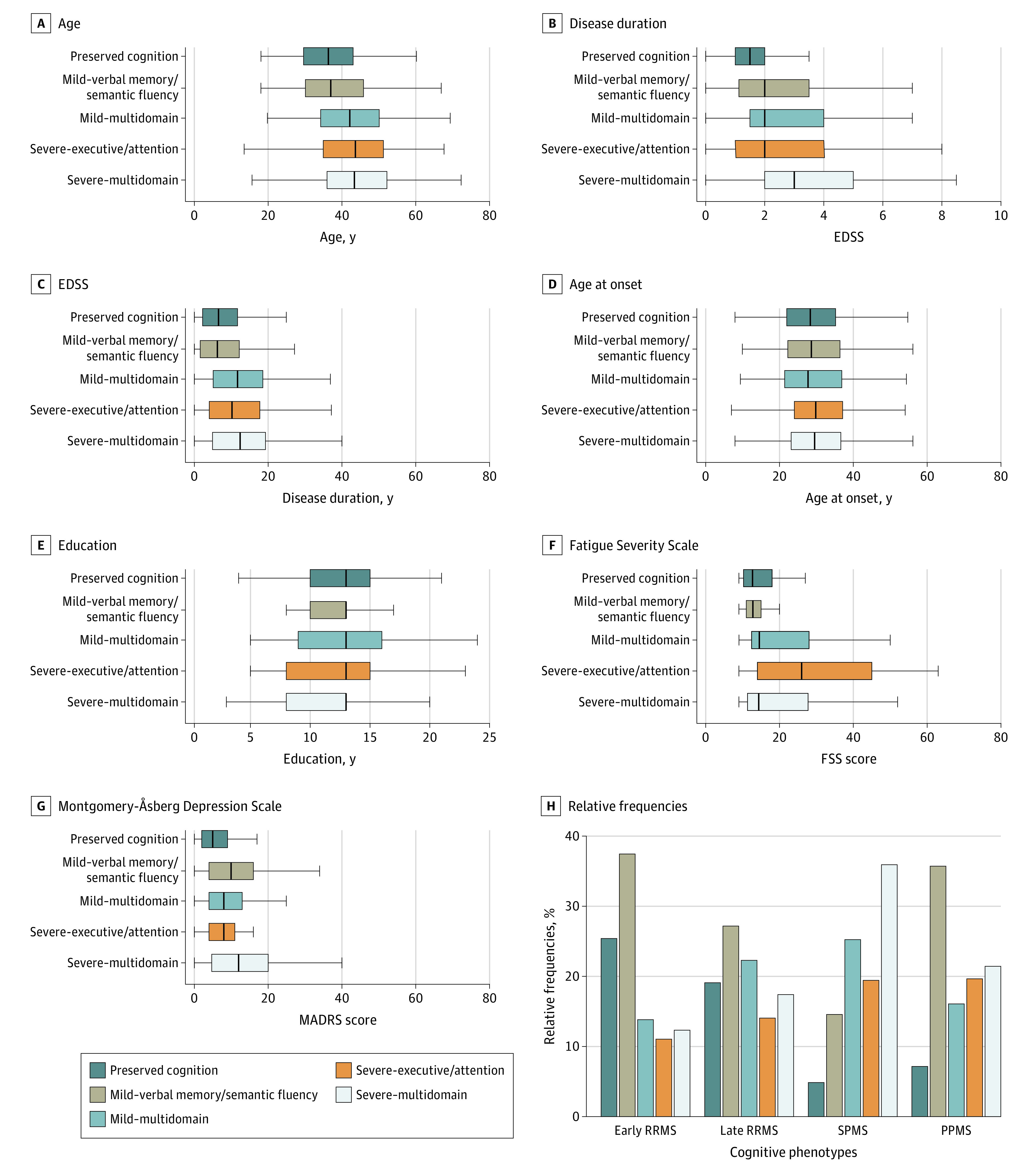
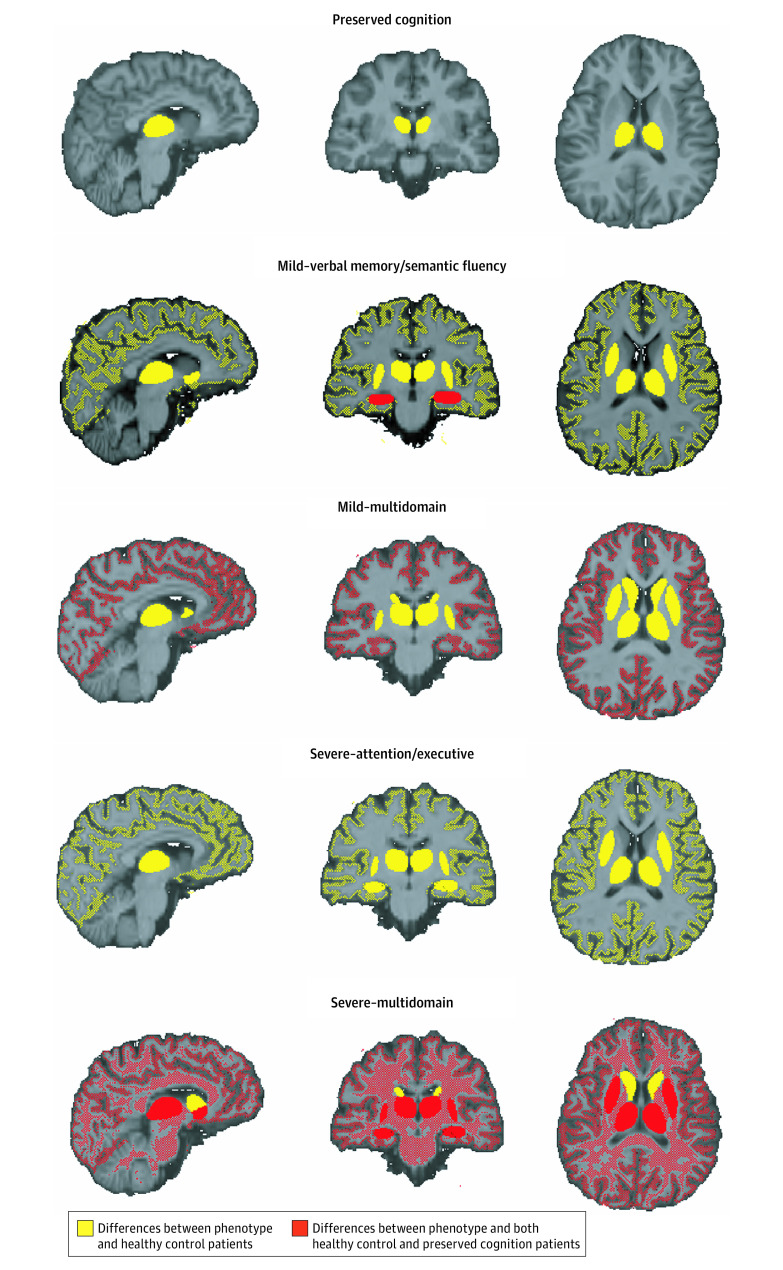
Results: A total of 1212 patients with MS (mean [SD] age, 41.1 [11.1] years; 784 women [64.7%]) and 196 healthy control individuals (mean [SD] age, 40.4 [8.6] years; 130 women [66.3%]) were analyzed in this study. Five cognitive phenotypes were identified: preserved cognition (n = 235 patients [19.4%]), mild-verbal memory/semantic fluency (n = 362 patients [29.9%]), mild-multidomain (n = 236 patients [19.5%]), severe-executive/attention (n = 167 patients [13.8%]), and severe-multidomain (n = 212 patients [17.5%]) involvement. Patients with preserved cognition and mild-verbal memory/semantic fluency were younger (mean [SD] age, 36.5 [9.8] years and 38.2 [11.1] years) and had shorter disease duration (mean [SD] 8.0 [7.3] years and 8.3 [7.6] years) compared with patients with mild-multidomain (mean [SD] age, 42.6 [11.2] years; mean [SD] disease duration, 12.8 [9.6] years; P < .001), severe-executive/attention (mean [SD] age, 42.9 [11.7] years; mean [SD] disease duration, 12.2 [9.5] years; P < .001), and severe-multidomain (mean [SD] age, 44.0 [11.0] years; mean [SD] disease duration, 13.3 [10.2] years; P < .001) phenotypes. Severe cognitive phenotypes prevailed in patients with progressive MS. At MRI evaluation, compared with those with preserved cognition, patients with mild-verbal memory/semantic fluency exhibited decreased mean (SE) hippocampal volume (5.42 [0.68] mL vs 5.13 [0.68] mL; P = .04), patients with the mild-multidomain phenotype had decreased mean (SE) cortical gray matter volume (687.69 [35.40] mL vs 662.59 [35.48] mL; P = .02), patients with severe-executive/attention had higher mean (SE) T2-hyperintense lesion volume (51.33 [31.15] mL vs 99.69 [34.07] mL; P = .04), and patients with the severe-multidomain phenotype had extensive brain damage, with decreased volume in all the brain structures explored, except for nucleus pallidus, amygdala and caudate nucleus.
Conclusions and relevance: This study found that by defining homogeneous and clinically meaningful phenotypes, the limitations of the traditional dichotomous classification in MS can be overcome. These phenotypes can represent a more meaningful measure of the cognitive status of patients with MS and can help define clinical disability, support clinicians in treatment choices, and tailor cognitive rehabilitation strategies.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
