

Predictors of postoperative biochemical remission in acromegaly
- PMID: 33394265
- PMCID: PMC10077515
- DOI: 10.1007/s11060-020-03669-4
Predictors of postoperative biochemical remission in acromegaly
Abstract
Purpose: Acromegaly is a rare neuroendocrine condition that can lead to significant morbidity. Despite China's vast population size, studies on acromegaly remain sparse. This study aimed to investigate the clinical characteristics and predictors of biochemical remission after surgery for acromegaly using the China Acromegaly Patient Association (CAPA) database.
Methods: A retrospective nationwide study was conducted using patient-reported data from CAPA database between 1998 and 2018. The principal component analysis (PCA) and logistic regression analysis were employed to determine independent predictors of biochemical remission at 3 months in patients after surgery.
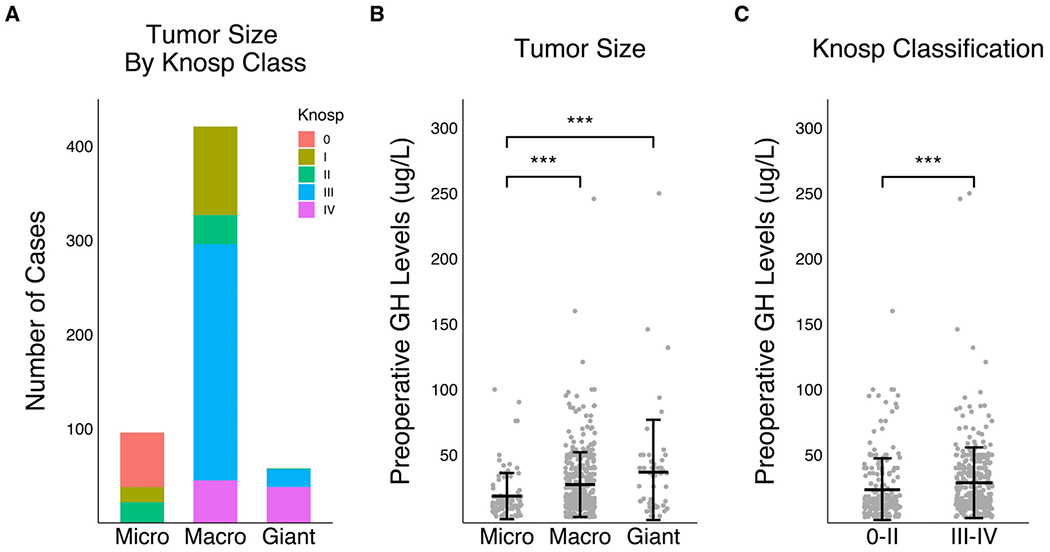
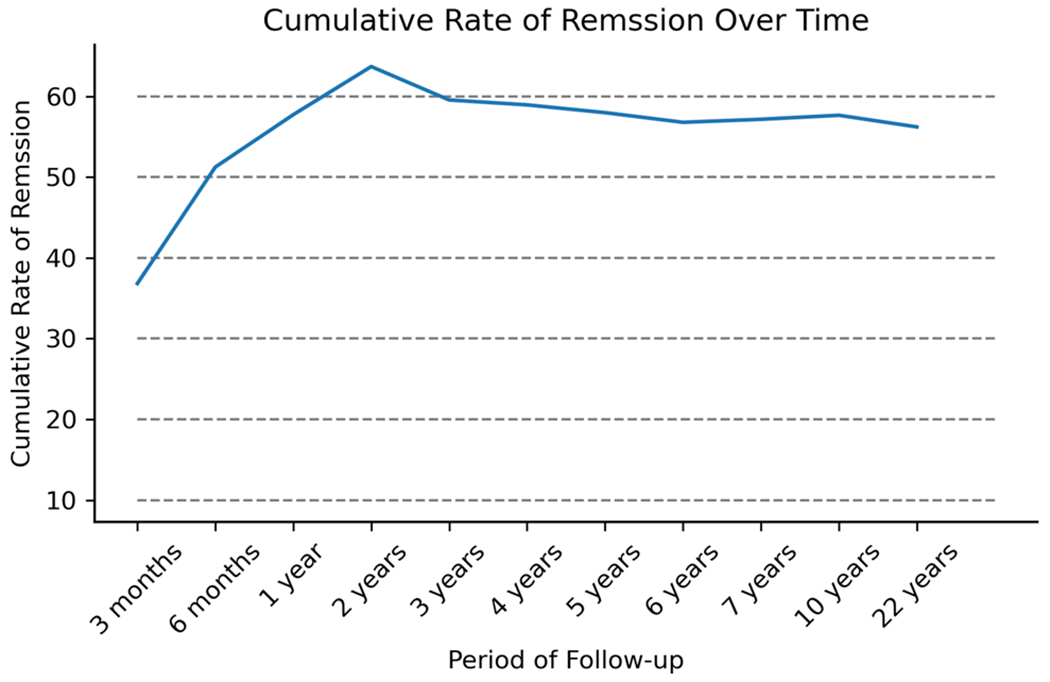
Results: Of the 546 surgical cases (mean age: 36.8 years; 59.5% females), macroadenomas and invasive tumors (Knosp score 3-4) were 83.9% and 64.1%, respectively. Ninety-five percent of patients were treated with endonasal surgery and 36.8% exhibited biochemical remission at 3-months postoperatively. The following independent predictors of biochemical remission were identified: preoperative growth hormone (GH) levels between 12 and 28 μg/L [odds ratio (OR) = 0.58; 95% confidence interval (CI), 0.37-0.92; p = 0.021], preoperative GH levels > 28 μg/L (OR = 0.55; 95% CI, 0.34-0.88; p = 0.013), macroadenoma (OR = 0.56; 95% CI, 0.32-0.96; p = 0.034), giant adenomas (OR = 0.14; 95% CI, 0.05-0.38; p < 0.001), Knosp score 3-4 (OR = 0.37; 95% CI, 0.24-0.57; p < 0.001), and preoperative medication usage (OR = 2.32; 95% CI, 1.46-3.70; p < 0.001).
Conclusions: In this nationwide study spanning over two decades, we highlight that higher preoperative GH levels, large tumor size, and greater extent of tumor invasiveness are associated with a lower likelihood of biochemical remission at 3-months after surgery, while preoperative medical therapy increases the chance of remission.
Keywords: Acromegaly; Biochemical remission; Growth hormone; Pituitary tumor; Predictors.
Conflict of interest statement
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
