

Cardiotoxicity during long-term trastuzumab use in patients with HER2-positive metastatic breast cancer: who needs cardiac monitoring?
- PMID: 33394273
- PMCID: PMC8019427
- DOI: 10.1007/s10549-020-06039-w
Cardiotoxicity during long-term trastuzumab use in patients with HER2-positive metastatic breast cancer: who needs cardiac monitoring?
Abstract
Purpose: Patients with HER2-positive metastatic breast cancer (MBC) usually receive many years of trastuzumab treatment. It is unknown whether these patients require continuous left ventricular ejection fraction (LVEF) monitoring. We studied a real-world cohort to identify risk factors for cardiotoxicity to select patients in whom LVEF monitoring could be omitted.
Methods: We included patients with HER2-positive MBC who received > 1 cycle of trastuzumab-based therapy in eight Dutch hospitals between 2000 and 2014. Cardiotoxicity was defined as LVEF < 50% that declined > 10%-points and was categorized into non-severe cardiotoxicity (LVEF 40-50%) and severe cardiotoxicity (LVEF < 40%). Multivariable Cox and mixed model analyses were performed to identify risk factors associated with cardiotoxicity. Additionally, we explored the reversibility of cardiotoxicity in patients who continued trastuzumab.
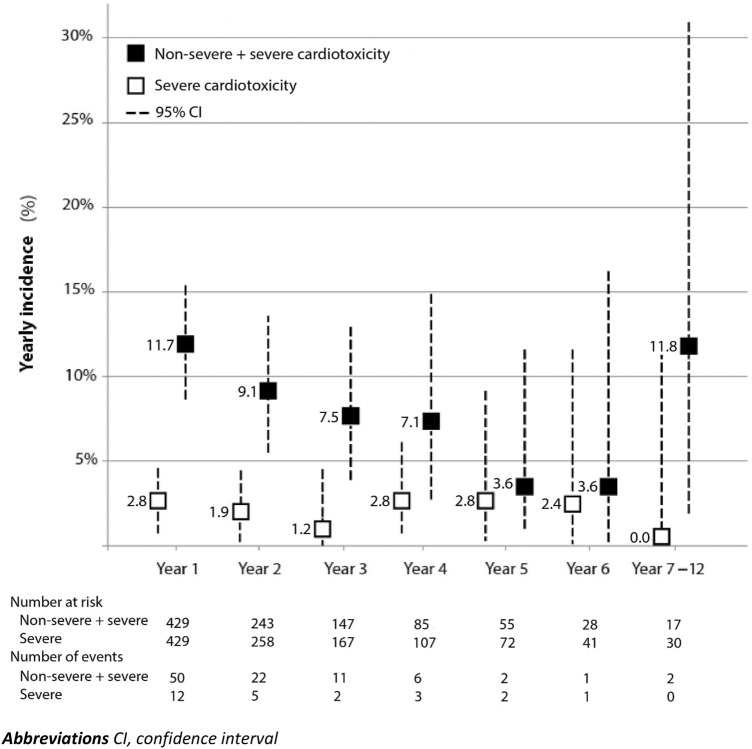
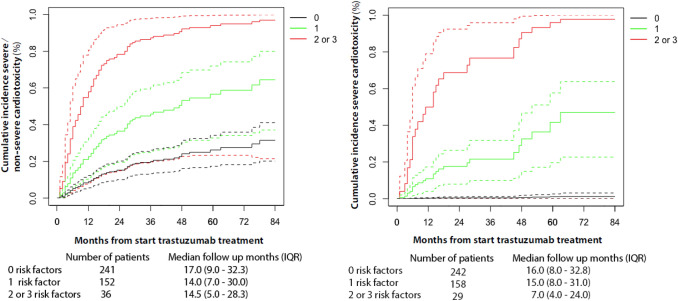
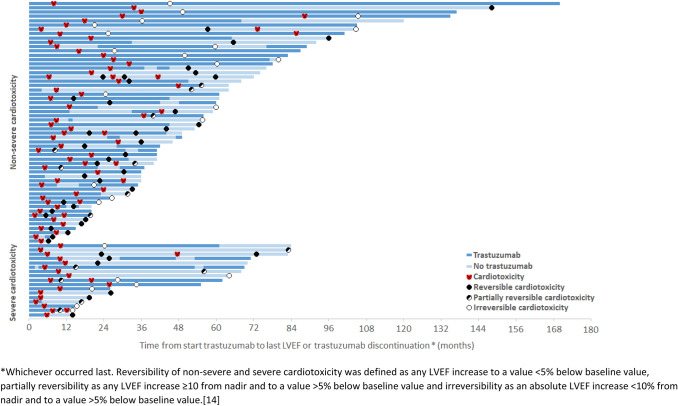
Results: In total, 429 patients were included. Median follow-up for cardiotoxicity was 15 months (interquartile range 8-31 months). The yearly incidence of non-severe + severe cardiotoxicity in the first and second year was 11.7% and 9.1%, respectively, which decreased thereafter. The yearly incidence of severe cardiotoxicity was low (2.8%) and stable over time. In non-smoking patients with baseline LVEF > 60% and no cardiotoxicity during prior neoadjuvant/adjuvant treatment, the cumulative incidence of severe cardiotoxicity was 3.1% after 4 years of trastuzumab. Despite continuing trastuzumab, LVEF decline was reversible in 56% of patients with non-severe cardiotoxicity and in 33% with severe cardiotoxicity.
Conclusions: Serial cardiac monitoring can be safely omitted in non-smoking patients with baseline LVEF > 60% and without cardiotoxicity during prior neoadjuvant/adjuvant treatment.
Keywords: Cardiotoxicity; HER2-positive metastatic breast cancer; LVEF monitoring; Screening for cardiotoxicity; Trastuzumab treatment.
Conflict of interest statement
TGS received funding from Memidis Pharma outside the current project. GSS has received institutional research funding from AstraZeneca, Merck, Novartis and Roche. The other authors have no relevant financial or non-financial interests to disclose.
Figures
References
-
- Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, Fleming T, Eiermann W, Wolter J, Pegram M, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344(11):783–792. doi: 10.1056/NEJM200103153441101. - DOI - PubMed
-
- Curigliano G, Lenihan D, Fradley M, Ganatra S, Barac A, Blaes A, Herrmann J, Porter C, Lyon AR, Lancellotti P, et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann Oncol. 2020;31(2):171–190. doi: 10.1016/j.annonc.2019.10.023. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
