

Sodium-Glucose Cotransporter-2 Inhibitors for Treatment of Nonalcoholic Fatty Liver Disease: A Meta-Analysis of Randomized Controlled Trials
- PMID: 33396949
- PMCID: PMC7823667
- DOI: 10.3390/metabo11010022
Sodium-Glucose Cotransporter-2 Inhibitors for Treatment of Nonalcoholic Fatty Liver Disease: A Meta-Analysis of Randomized Controlled Trials
Abstract
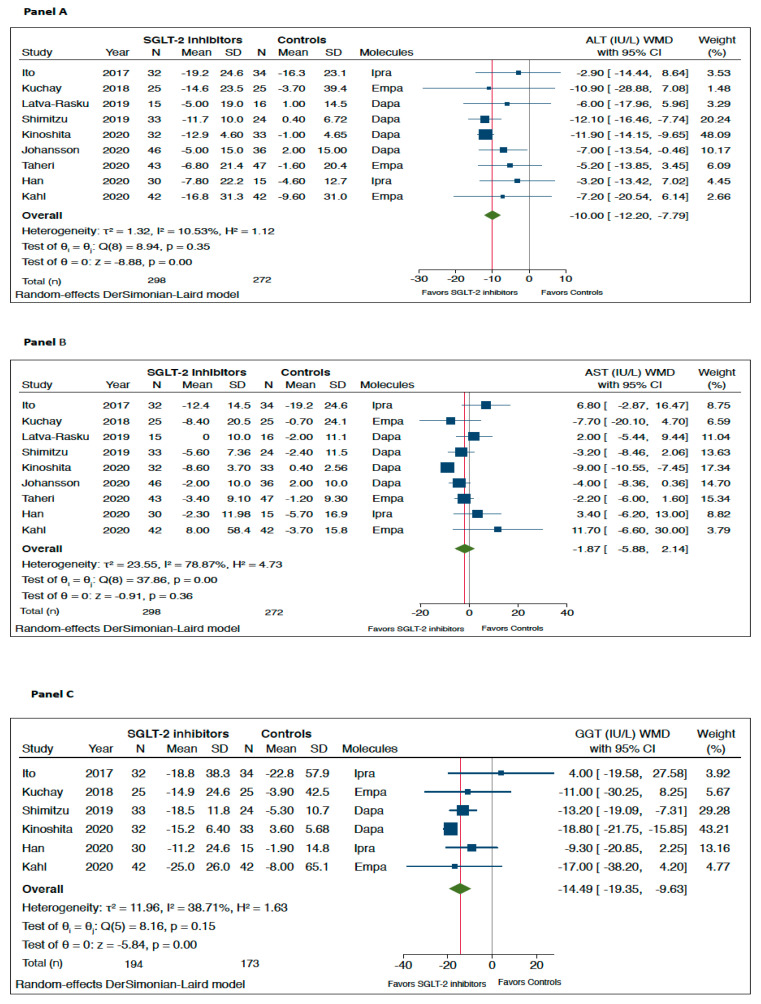
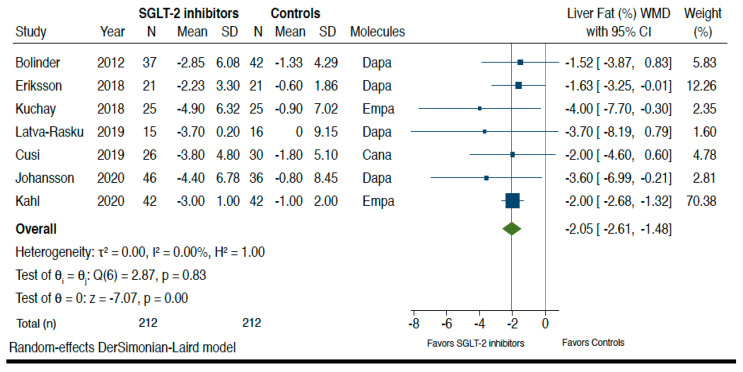
Recent randomized controlled trials (RCTs) tested the efficacy of sodium-glucose cotransporter-2 (SGLT-2) inhibitors to specifically treat nonalcoholic fatty liver disease (NAFLD). We systematically searched three electronic databases (up to 31 October 2020) for identifying placebo-controlled or head-to-head RCTs that used SGLT-2 inhibitors for treatment of NAFLD. No published RCTs with paired liver biopsy data were available for the meta-analysis. Primary outcome measures were changes in serum liver enzyme levels and liver fat content on imaging techniques. Overall, we included a total of twelve RCTs testing the efficacy of dapagliflozin (n = six RCTs), empagliflozin (n = three RCTs), ipragliflozin (n = two RCTs) or canagliflozin (n = one RCT) to specifically treat NAFLD for a median period of 24 weeks with aggregate data on 850 middle-aged overweight or obese individuals with NAFLD (90% with type 2 diabetes). Compared to placebo/reference therapy, treatment with SGLT-2 inhibitors significantly decreased serum alanine aminotransferase (weighted mean differences (WMD): -10.0 IU/L, 95%CI -12.2 to -7.79 IU/L; I2 = 10.5%) and gamma-glutamyltransferase levels (WMD: -14.49 IU/L, 95%CI -19.35 to -9.63 IU/L, I2 = 38.7%), as well as the absolute percentage of liver fat content on magnetic resonance-based techniques (WMD: -2.05%, 95%CI -2.61 to -1.48%; I2 = 0%). In conclusion, SGLT-2 inhibitors seem to be a promising treatment option for NAFLD.
Keywords: NAFLD; SGLT-2 inhibitors; nonalcoholic fatty liver disease; nonalcoholic steatohepatitis; nonalcoholic steatohepatitis (NASH); type 2 diabetes mellitus.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Non-alcoholic Fatty Liver Disease Study Group. Lonardo A., Bellentani S., Argo C.K., Ballestri S., Byrne C.D., Caldwell S.H., Cortez-Pinto H., Grieco A., Machado M.V., et al. Epidemiological modifiers of non-alcoholic fatty liver disease: Focus on high-risk groups. Dig. Liver Dis. 2015;47:997–1006. doi: 10.1016/j.dld.2015.08.004. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
