

Feasibility of mesentericoportal vein reconstruction by autologous falciform ligament during pancreaticoduodenectomy-cohort study
- PMID: 33397346
- PMCID: PMC7783990
- DOI: 10.1186/s12893-020-01019-9
Feasibility of mesentericoportal vein reconstruction by autologous falciform ligament during pancreaticoduodenectomy-cohort study
Abstract
Background: Mesentericoportal vein (MPV) resection in pancreatic ductal adenocarcinoma (PDAC) surgery has become a common procedure. A few studies had described the use of falciform ligament (FL) for MPV reconstruction and received encouraging preliminary effects.
Aims: This study was designed to explore the feasibility and efficacy of this technique compared with others.
Methods: Patients who underwent pancreaticoduodenectomy (PD) with MPV resection for PDAC from 2009 to 2018 were enrolled. Medical records were retrospectively reviewed, MPV reconstructions using FL were distinguished and compared with other techniques.
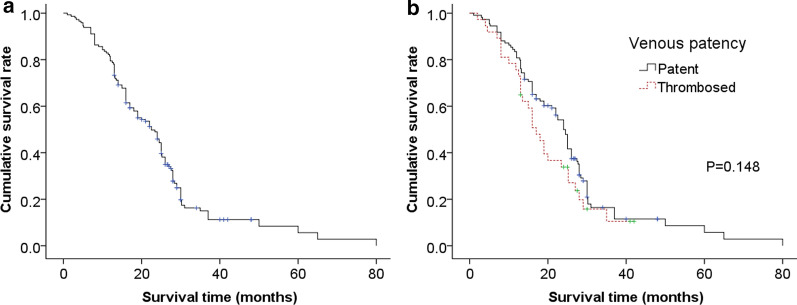
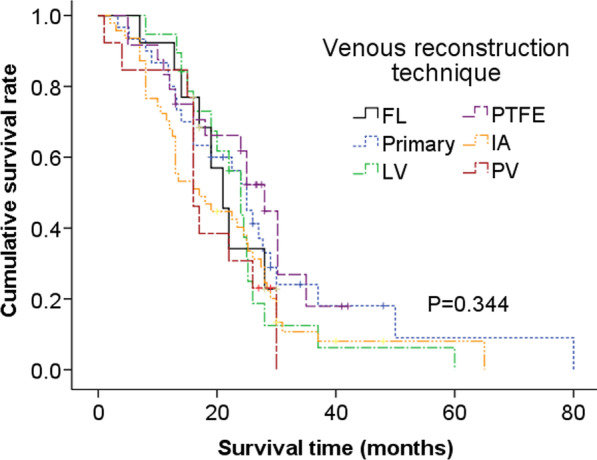
Results: 146 patients underwent MPV reconstruction, and 13 received FL venoplasty. Other reconstruction techniques included primary end-to-end anastomosis (primary, n = 30), lateral venorrhaphy (LV, n = 19), polytetrafluoroethylene conduit interposition (PTFE, n = 24), iliac artery (IA) allografts interposition (n = 47), and portal vein (PV) allografts interposition (n = 13). FL group holds the advantages of shortest operation time (p = 0.023), lowest blood loss (p = 0.109), and shortest postoperative hospital stay (p = 0.125). The grouped patency rates of FL, primary, LV, PTFE, IA, and PV were 100%, 90%, 68%, 54%, 68%, and 85% respectively. Comparison displayed that FL had the highest patency rate (p = 0.008) and lowest antiplatelet/anticoagulation proportion (p = 0.000). Complications and long-term survival were similar among different techniques. The median survival time of patent group (24.0 months, 95% CI: 22.0-26.0) was much longer than that of the thrombosed (17.0 months, 95% CI: 13.7-20.3), though without significant difference (P = 0.148).
Conclusions: PD with MPV resection and reconstruction by FL is safe, feasible, and efficacious, it might provide a potential benefit for patients.
Keywords: Falciform ligament; Pancreatic cancer; Patency; Survival; Venous reconstruction technique.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Grants and funding
- 2019-I2M-5-030/Research Unit Project of Chinese Academy of Medical Sciences
- 81770645/National Natural Science Foundation of China
- 2018260134/National Health and Family Planning Commission of China
- 2020C03057/Key Research and Development Program of Zhejiang Province
- LGF18H030006/Basic Public Interest Research Project of Zhejiang Province
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
