

Short and long-term impact of four sets of actions on acute ischemic stroke management in Rhône County, a population based before-and-after prospective study
- PMID: 33397363
- PMCID: PMC7783982
- DOI: 10.1186/s12913-020-05982-0
Short and long-term impact of four sets of actions on acute ischemic stroke management in Rhône County, a population based before-and-after prospective study
Abstract
Background: Optimizing access to recanalization therapies in acute ischemic stroke patients is crucial. Our aim was to measure the short and long term effectiveness, at the acute phase and 1 year after stroke, of four sets of actions implemented in the Rhône County.
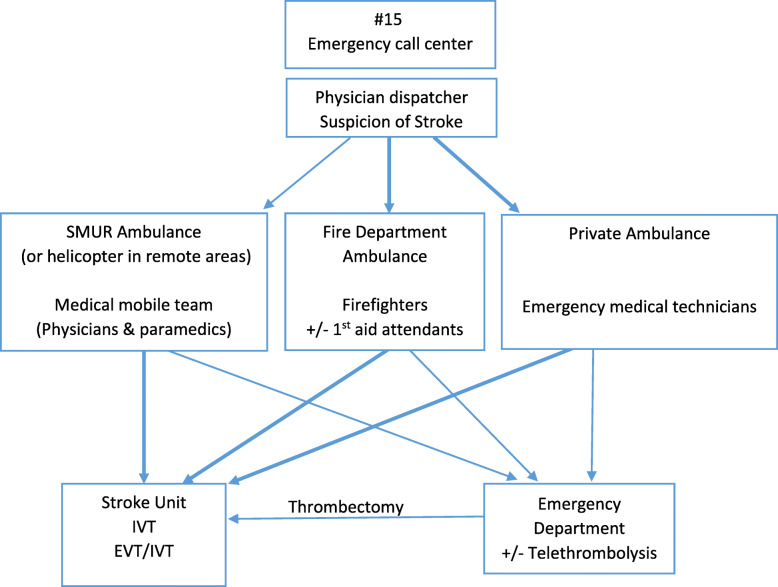
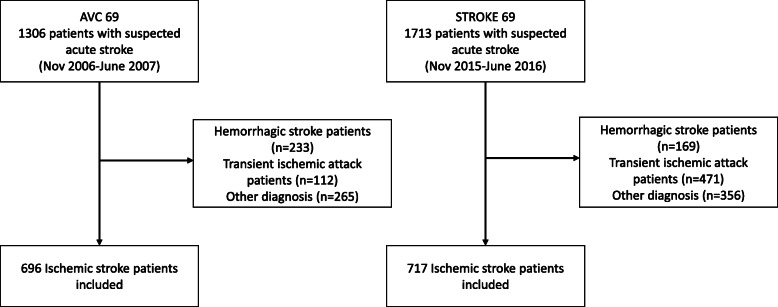
Methods: The four multilevel actions were 1) increase in stroke units bed capacity and development of endovascular therapy; 2) improvement in knowledge and skills of healthcare providers involved in acute stroke management using a bottom-up approach; 3) development and implementation of new organizations (transportation routes, pre-notification, coordination by the emergency call center physician dispatcher); and 4) launch of regional public awareness campaigns in addition to national campaigns. A before-and-after study was conducted with two identical population-based cohort studies in 2006-7 and 2015-16 in all adult ischemic stroke patients admitted to any emergency department or stroke unit of the Rhône County. The primary outcome criterion was in-hospital management times, and the main secondary outcome criteria were access to reperfusion therapy (either intravenous thrombolysis or endovascular treatment) and pre-hospital management times in the short term, and 12-month prognosis measured by the modified Rankin Scale (mRS) in the long term.
Results: Between 2015-16 and 2006-7 periods ischemic stroke patients increased from 696 to 717, access to reperfusion therapy increased from 9 to 23% (p < 0.0001), calls to emergency call-center from 40 to 68% (p < 0.0001), first admission in stroke unit from 8 to 30% (p < 0.0001), and MRI within 24 h from 18 to 42% (p < 0.0001). Onset-to-reperfusion time significantly decreased from 3h16mn [2 h54-4 h05] to 2h35mn [2 h05-3 h19] (p < 0.0001), mainly related to a decrease in delay from admission to imaging. A significant decrease of disability was observed, as patients with mild disability (mRS [0-2]) at 12 months increased from 48 to 61% (p < 0.0001). Pre-hospital times, however, did not change significantly.
Conclusions: We observed significant improvement in access to reperfusion therapy, mainly through a strong decrease of in-hospital management times, and in 12-month disability after the implementation of four sets of actions between 2006 and 2016 in the Rhône County. Reducing pre-hospital times remains a challenge.
Keywords: Cohort study; Emergency medical services; Health services research; Ischemic stroke; Organization; Reperfusion therapy; Time-to-treatment.
Conflict of interest statement
The authors declare no conflict of interest regarding this study.
Figures
References
-
- Lansberg MG, Schrooten M, Bluhmki E, Thijs VN, Saver JL. Treatment time-specific number needed to treat estimates for tissue plasminogen activator therapy in acute stroke based on shifts over the entire range of the modified Rankin scale. Stroke. 2009;40:2079–2084. doi: 10.1161/STROKEAHA.108.540708. - DOI - PMC - PubMed
-
- Lees KR, Bluhmki E, von Kummer R, Brott TG, Toni D, Grotta JC, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet Lond Engl. 2010;375:1695–1703. doi: 10.1016/S0140-6736(10)60491-6. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
