

Vaccination strategies for measles control and elimination: time to strengthen local initiatives
- PMID: 33397366
- PMCID: PMC7781821
- DOI: 10.1186/s12916-020-01843-z
Vaccination strategies for measles control and elimination: time to strengthen local initiatives
Abstract
Background: Through a combination of strong routine immunization (RI), strategic supplemental immunization activities (SIA) and robust surveillance, numerous countries have been able to approach or achieve measles elimination. The fragility of these achievements has been shown, however, by the resurgence of measles since 2016. We describe trends in routine measles vaccine coverage at national and district level, SIA performance and demographic changes in the three regions with the highest measles burden.
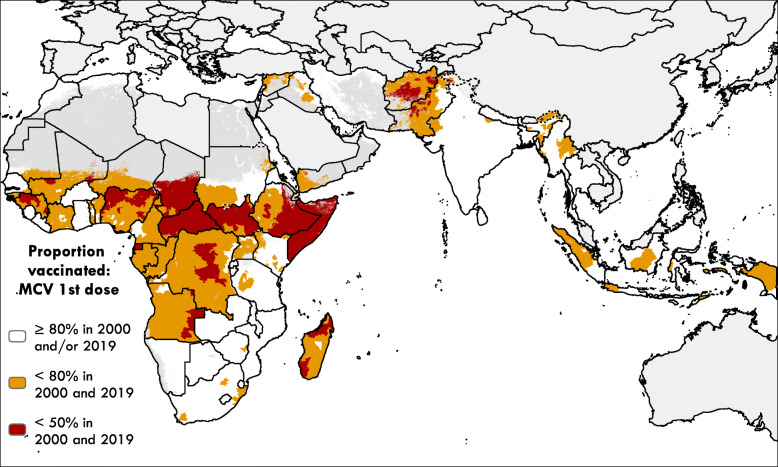
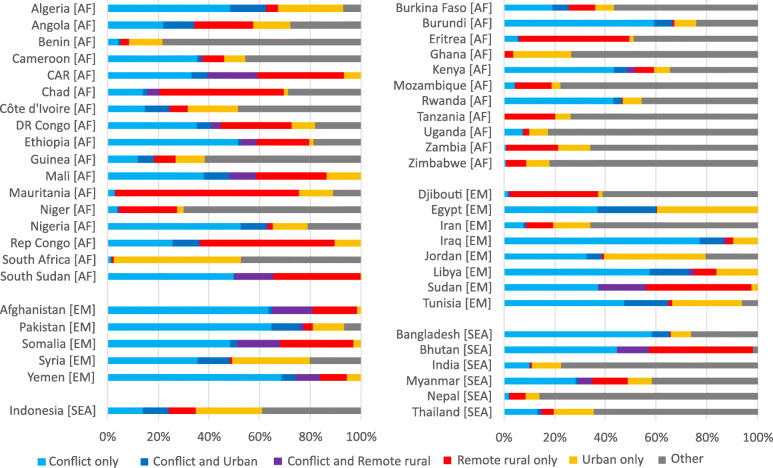
Findings: WHO-UNICEF estimates of immunization coverage show that global coverage of the first dose of measles vaccine has stabilized at 85% from 2015 to 19. In 2000, 17 countries in the WHO African and Eastern Mediterranean regions had measles vaccine coverage below 50%, and although all increased coverage by 2019, at a median of 60%, it remained far below levels needed for elimination. Geospatial estimates show many low coverage districts across Africa and much of the Eastern Mediterranean and southeast Asian regions. A large proportion of children unvaccinated for MCV live in conflict-affected areas with remote rural areas and some urban areas also at risk. Countries with low RI coverage use SIAs frequently, yet the ideal timing and target age range for SIAs vary within countries, and the impact of SIAs has often been mitigated by delays or disruptions. SIAs have not been sufficient to achieve or sustain measles elimination in the countries with weakest routine systems. Demographic changes also affect measles transmission, and their variation between and within countries should be incorporated into strategic planning.
Conclusions: Rebuilding services after the COVID-19 pandemic provides a need and an opportunity to increase community engagement in planning and monitoring services. A broader suite of interventions is needed beyond SIAs. Improved methods for tracking coverage at the individual and community level are needed together with enhanced surveillance. Decision-making needs to be decentralized to develop locally-driven, sustainable strategies for measles control and elimination.
Keywords: Campaigns; Elimination; Measles; Routine immunization.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Measles vaccines: WHO position paper – April 2017. Wkly Epidemiol Rec 2017; 92: 205–227. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
