

Protective reactive thymus hyperplasia in COVID-19 acute respiratory distress syndrome
- PMID: 33397460
- PMCID: PMC7781174
- DOI: 10.1186/s13054-020-03440-1
Protective reactive thymus hyperplasia in COVID-19 acute respiratory distress syndrome
Abstract
Background: Patients with COVID-19 (COVID) may develop acute respiratory distress syndrome with or without sepsis, coagulopathy and visceral damage. While chest CT scans are routinely performed in the initial assessment of patients with severe pulmonary forms, thymus involvement and reactivation have not been investigated so far.
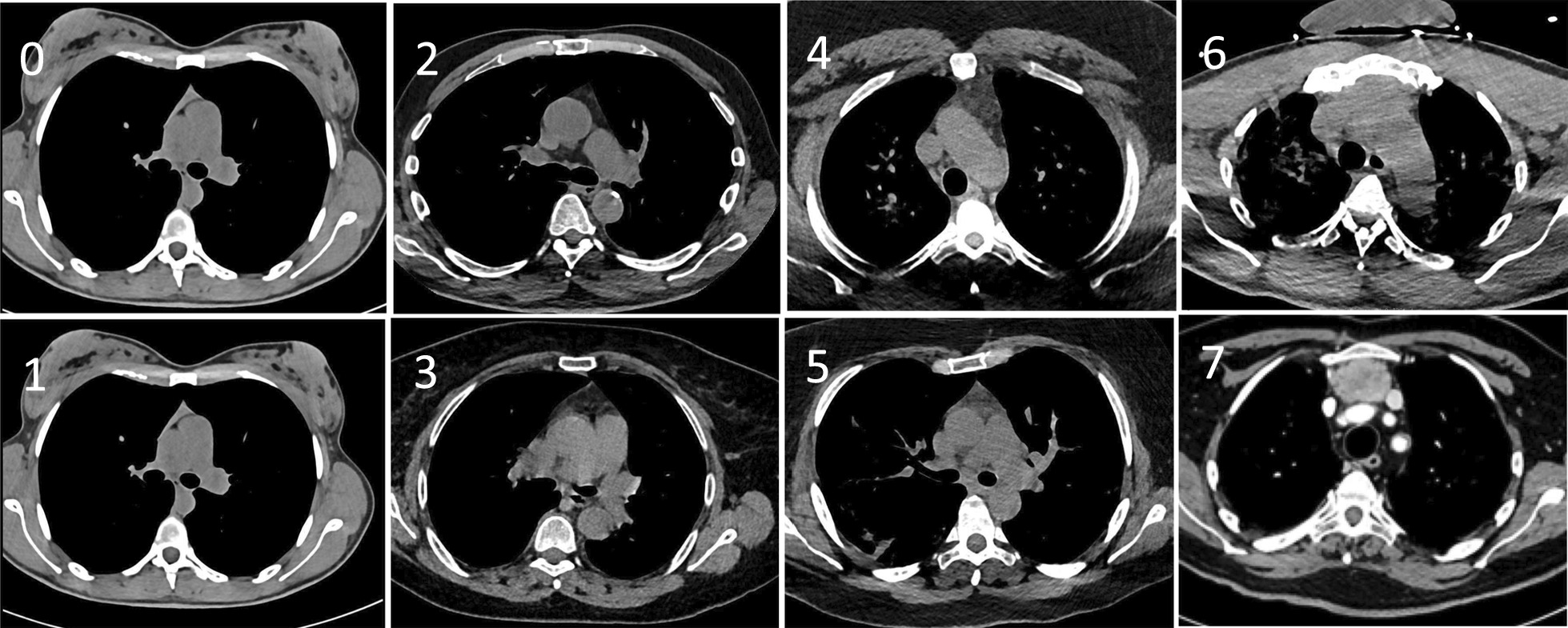
Methods: In this observational study, we systematically scored the enlargement of the thymus and the lung involvement, using CT scans, in all adult patients admitted to the ICU for COVID or any other cause (control group) at one centre between March and April 2020. Initial biological investigations included nasal detection of SARS-CoV-2 ribonucleic acid by polymerase chain reaction (PCR). In a subgroup of 24 patients with different degrees of pulmonary involvement and thymus hypertrophy, plasma cytokine concentrations were measured and the export of mature T cells from the thymus was estimated simultaneously by PCR quantification of T cell receptor excision circles (TRECs).
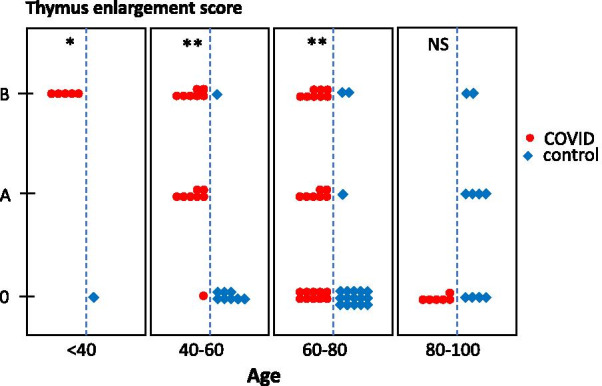
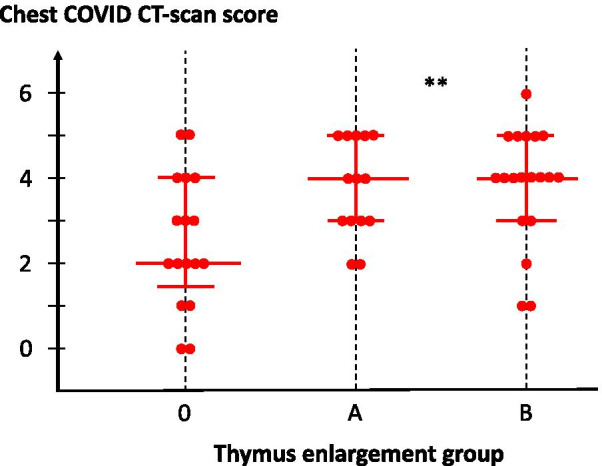
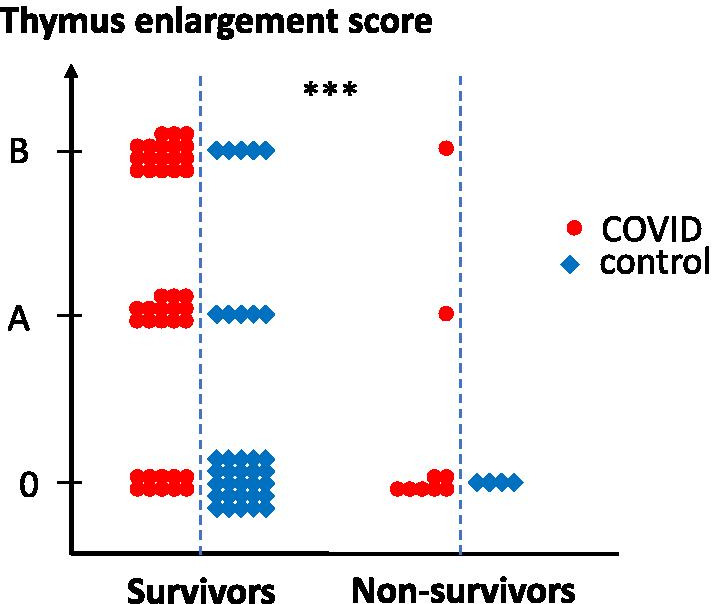
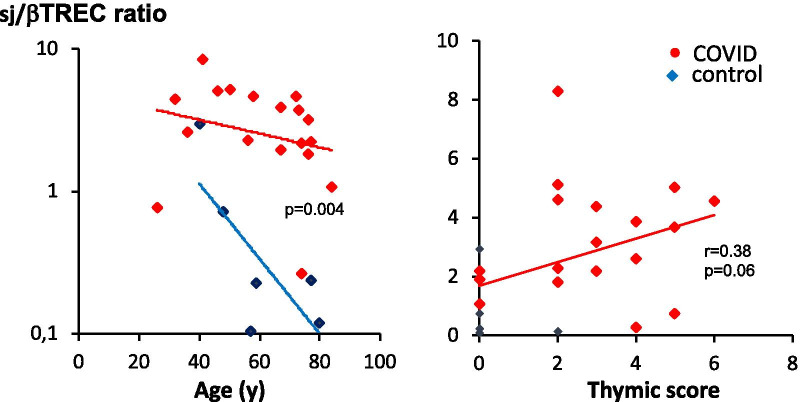
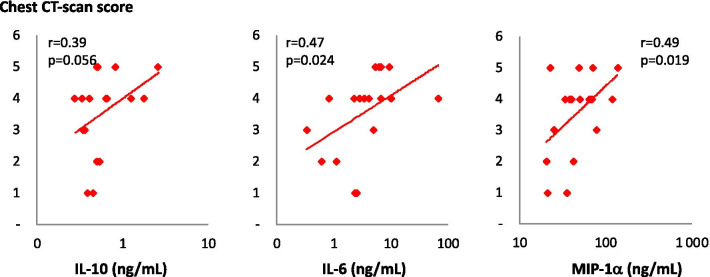
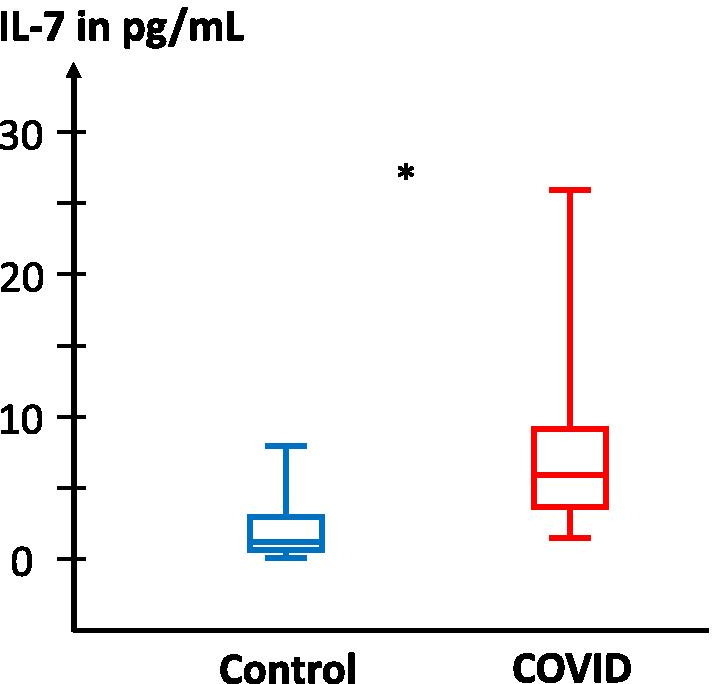
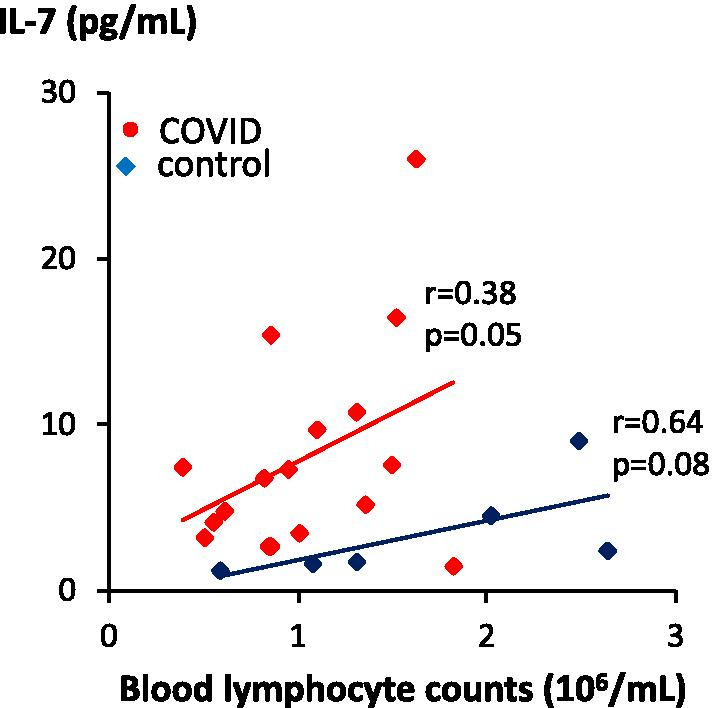
Results: Eighty-seven patients were studied: 50 COVID patients and 37 controls. Non-atrophic or enlarged thymus was more commonly observed in COVID patients than in controls (66% vs. 24%, p < 0.0001). Thymus enlargement in COVID patients was associated with more extensive lung injury score on CT scans (4 [3-5] vs. 2 [1.5-4], p = 0.01), but a lower mortality rate (8.6% vs. 41.2%, p < 0.001). Other factors associated with mortality were age, lymphopaenia, high CRP and co-morbidities. COVID patients had higher concentrations of IL-7 (6.00 [3.72-9.25] vs. 2.17 [1.76-4.4] pg/mL; p = 0.04) and higher thymic production of new lymphocytes (sj/βTREC ratio = 2.88 [1.98-4.51] vs. 0.23 [0.15-0.60]; p = 0.004). Thymic production was also correlated with the CT scan thymic score (r = 0.38, p = 0.03) and inversely correlated with the number of lymphocytes (r = 0.56, p = 0.007).
Conclusion: In COVID patients, thymus enlargement was frequent and associated with increased T lymphocyte production, which appears to be a beneficial adaptation to virus-induced lymphopaenia. The lack of thymic activity/reactivation in older SARS-CoV-2 infected patients could contribute to a worse prognosis.
Keywords: COVID-19; TREC; Thymus reactivation.
Conflict of interest statement
All authors declare no competing interests related to this study.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
