

Efficacy and Safety of Dulaglutide 3.0 mg and 4.5 mg Versus Dulaglutide 1.5 mg in Metformin-Treated Patients With Type 2 Diabetes in a Randomized Controlled Trial (AWARD-11)
- PMID: 33397768
- PMCID: PMC7896253
- DOI: 10.2337/dc20-1473
Efficacy and Safety of Dulaglutide 3.0 mg and 4.5 mg Versus Dulaglutide 1.5 mg in Metformin-Treated Patients With Type 2 Diabetes in a Randomized Controlled Trial (AWARD-11)
Abstract
Objective: To compare efficacy and safety of dulaglutide at doses of 3.0 and 4.5 mg versus 1.5 mg in patients with type 2 diabetes inadequately controlled with metformin.
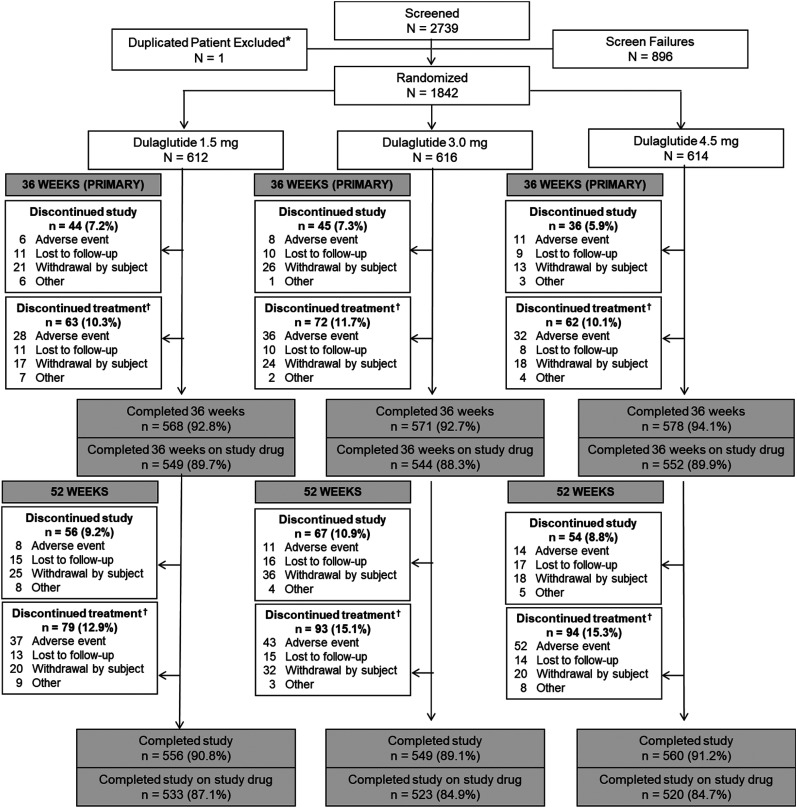
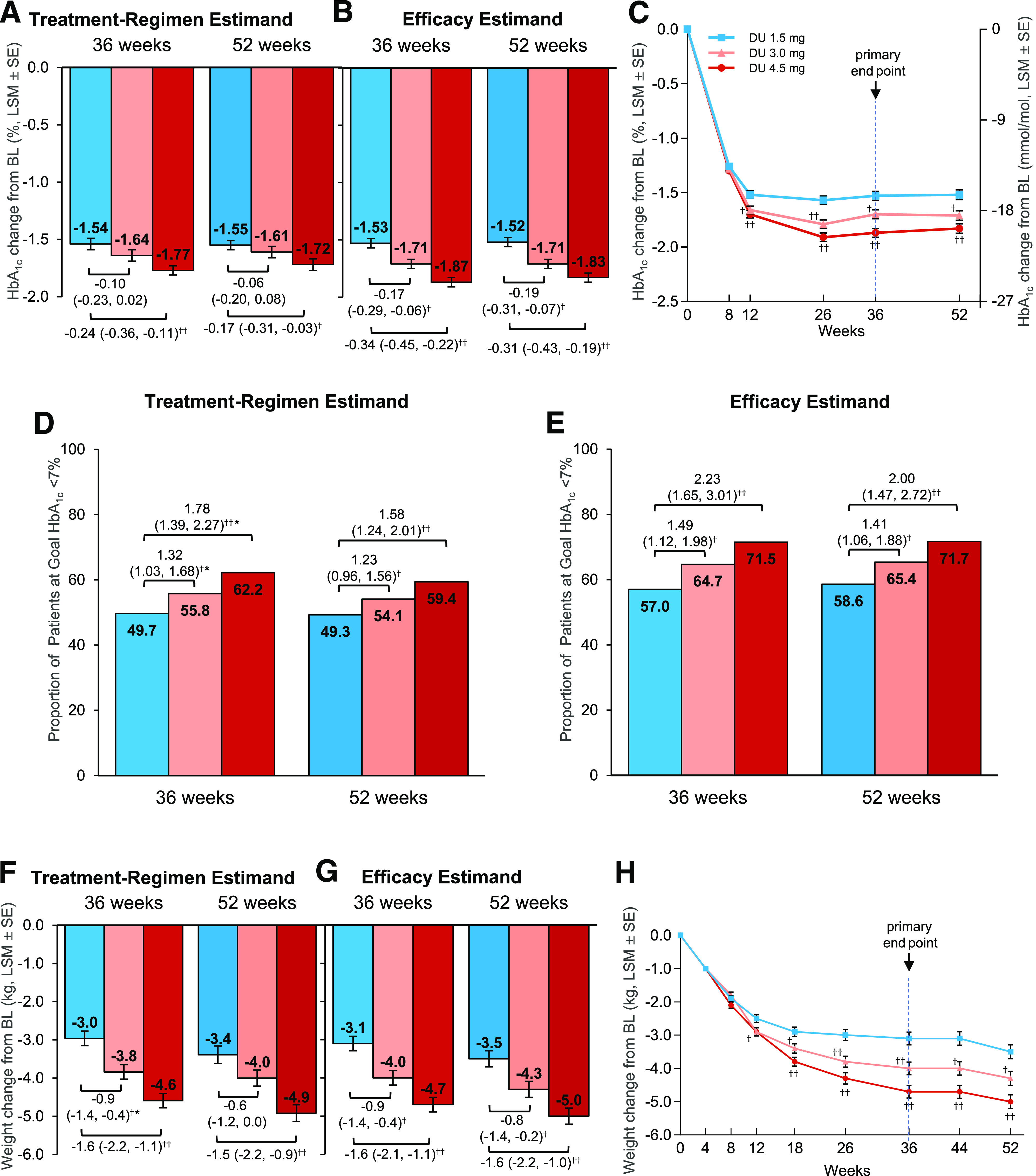
Research design and methods: Patients were randomly assigned to once-weekly dulaglutide 1.5 mg, 3.0 mg, or 4.5 mg for 52 weeks. The primary objective was determining superiority of dulaglutide 3.0 mg and/or 4.5 mg over 1.5 mg in HbA1c reduction at 36 weeks. Secondary superiority objectives included change in body weight. Two estimands addressed efficacy objectives: treatment regimen (regardless of treatment discontinuation or rescue medication) and efficacy (on treatment without rescue medication) in all randomly assigned patients.
Results: Mean baseline HbA1c and BMI in randomly assigned patients (N = 1,842) was 8.6% (70 mmol/mol) and 34.2 kg/m2, respectively. At 36 weeks, dulaglutide 4.5 mg provided superior HbA1c reductions compared with 1.5 mg (treatment-regimen estimand: -1.77 vs. -1.54% [-19.4 vs. -16.8 mmol/mol], estimated treatment difference [ETD] -0.24% (-2.6 mmol/mol), P < 0.001; efficacy estimand: -1.87 vs. -1.53% [-20.4 vs. -16.7 mmol/mol], ETD -0.34% (-3.7 mmol/mol), P < 0.001). Dulaglutide 3.0 mg was superior to 1.5 mg for reducing HbA1c, using the efficacy estimand (ETD -0.17% [-1.9 mmol/mol]; P = 0.003) but not the treatment-regimen estimand (ETD -0.10% [-1.1 mmol/mol]; P = 0.096). Dulaglutide 4.5 mg was superior to 1.5 mg for weight loss at 36 weeks for both estimands (treatment regimen: -4.6 vs. -3.0 kg, ETD -1.6 kg, P < 0.001; efficacy: -4.7 vs. -3.1 kg, ETD -1.6 kg, P < 0.001). Common adverse events through 36 weeks included nausea (1.5 mg, 13.4%; 3 mg, 15.6%; 4.5 mg, 16.4%) and vomiting (1.5 mg, 5.6%; 3 mg, 8.3%; 4.5 mg, 9.3%).
Conclusions: In patients with type 2 diabetes inadequately controlled by metformin, escalation from dulaglutide 1.5 mg to 3.0 mg or 4.5 mg provided clinically relevant, dose-related reductions in HbA1c and body weight with a similar safety profile.
Trial registration: ClinicalTrials.gov NCT03495102.
© 2021 by the American Diabetes Association.
Figures
References
-
- American Diabetes Association . 9. Pharmacologic approaches to glycemic treatment: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020;43(Suppl. 1):S98–S110 - PubMed
-
- Skrivanek Z, Gaydos BL, Chien JY, et al. . Dose-finding results in an adaptive, seamless, randomized trial of once-weekly dulaglutide combined with metformin in type 2 diabetes patients (AWARD-5). Diabetes Obes Metab 2014;16:748–756 - PubMed
-
- Kristensen SL, Rørth R, Jhund PS, et al. . Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol 2019;7:776–785 - PubMed
-
- Egan AG, Blind E, Dunder K, et al. . Pancreatic safety of incretin-based drugs--FDA and EMA assessment. N Engl J Med 2014;370:794–797 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
