

Cell Therapy for Chronic TBI: Interim Analysis of the Randomized Controlled STEMTRA Trial
- PMID: 33397772
- PMCID: PMC8055341
- DOI: 10.1212/WNL.0000000000011450
Cell Therapy for Chronic TBI: Interim Analysis of the Randomized Controlled STEMTRA Trial
Abstract
Objective: To determine whether chronic motor deficits secondary to traumatic brain injury (TBI) can be improved by implantation of allogeneic modified bone marrow-derived mesenchymal stromal/stem cells (SB623).
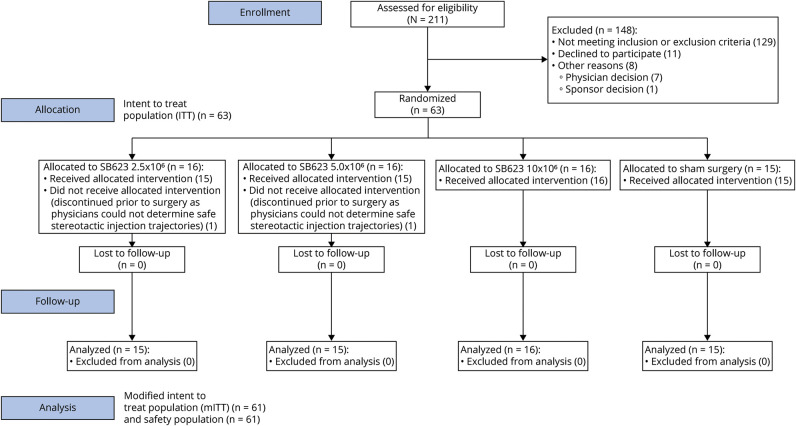
Methods: This 6-month interim analysis of the 1-year double-blind, randomized, surgical sham-controlled, phase 2 Stem Cell Therapy for Traumatic Brain Injury (STEMTRA) trial (NCT02416492) evaluated safety and efficacy of the stereotactic intracranial implantation of SB623 in patients with stable chronic motor deficits secondary to TBI. Patients in this multicenter trial (n = 63) underwent randomization in a 1:1:1:1 ratio to 2.5 × 106, 5.0 × 106, or 10 × 106 SB623 cells or control. Safety was assessed in patients who underwent surgery (n = 61), and efficacy was assessed in the modified intent-to-treat population of randomized patients who underwent surgery (n = 61; SB623 = 46, control = 15).
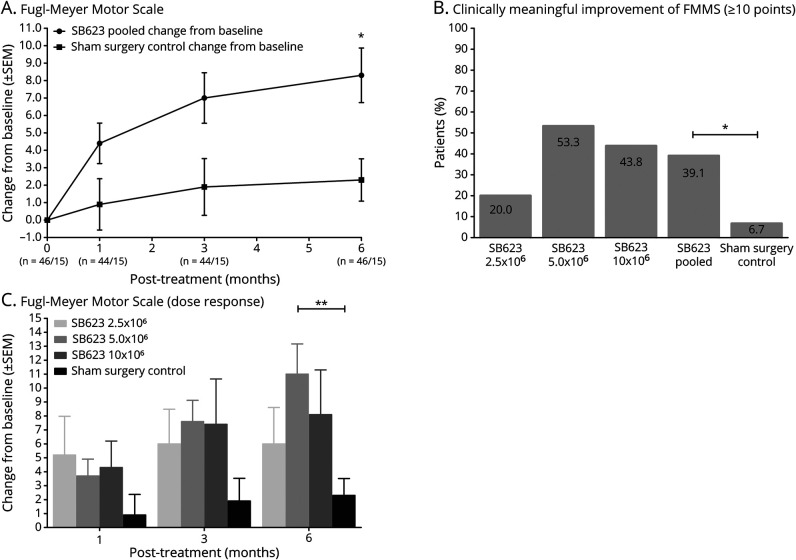
Results: The primary efficacy endpoint of significant improvement from baseline of Fugl-Meyer Motor Scale score at 6 months for SB623-treated patients was achieved. SB623-treated patients improved by (least square [LS] mean) 8.3 (standard error 1.4) vs 2.3 (standard error 2.5) for control at 6 months, the LS mean difference was 6.0 (95% confidence interval 0.3-11.8, p = 0.040). Secondary efficacy endpoints improved from baseline but were not statistically significant vs control at 6 months. There were no dose-limiting toxicities or deaths, and 100% of SB623-treated patients experienced treatment-emergent adverse events vs 93.3% of control patients (p = 0.25).
Conclusions: SB623 cell implantation appeared to be safe and well tolerated, and patients implanted with SB623 experienced significant improvement from baseline motor status at 6 months compared to controls.
Clinicaltrialsgov identifier: NCT02416492.
Classification of evidence: This study provides Class I evidence that implantation of SB623 was well tolerated and associated with improvement in motor status.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
Traumatic Brain Injury: A Success Stemming From Stem Cells.Neurology. 2021 Feb 22;96(8):357-358. doi: 10.1212/WNL.0000000000011455. Neurology. 2021. PMID: 33408142 No abstract available.
-
Stem cell implants show promise in chronic traumatic brain injury.Nat Rev Neurol. 2021 Feb;17(2):64. doi: 10.1038/s41582-021-00459-y. Nat Rev Neurol. 2021. PMID: 33432162 No abstract available.
Comment on
-
Traumatic Brain Injury: A Success Stemming From Stem Cells.Neurology. 2021 Feb 22;96(8):357-358. doi: 10.1212/WNL.0000000000011455. Neurology. 2021. PMID: 33408142 No abstract available.
References
-
- James SL, Theadom A, Ellenbogen RG; GBD 2016 Traumatic Brain Injury and Spinal Cord Injury Collaborators. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2019;18:56–87. - PMC - PubMed
-
- Selassie AW, Zaloshnja E, Langlois JA, Miller T, Jones P, Steiner C. Incidence of long-term disability following traumatic brain injury hospitalization, United States, 2003. J Head Trauma Rehabil 2008;23:123–131. - PubMed
-
- Thurman DJ, Alverson C, Dunn KA, Guerrero J, Sniezek JE. Traumatic brain injury in the United States: a public health perspective. J Head Trauma Rehabil 1999;14:602–615. - PubMed
-
- Walker WC, Pickett TC. Motor impairment after severe traumatic brain injury: a longitudinal multicenter study. J Rehabil Res Dev 2007;44:975–982. - PubMed
-
- Seledtsov VI, Rabinovich SS, Parlyuk OV, et al. Cell transplantation therapy in re-animating severely head-injured patients. Biomed Pharmacother 2005;59:415–420. - PubMed
Publication types
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials