

Brown adipose tissue is associated with cardiometabolic health
- PMID: 33398160
- PMCID: PMC8461455
- DOI: 10.1038/s41591-020-1126-7
Brown adipose tissue is associated with cardiometabolic health
Abstract
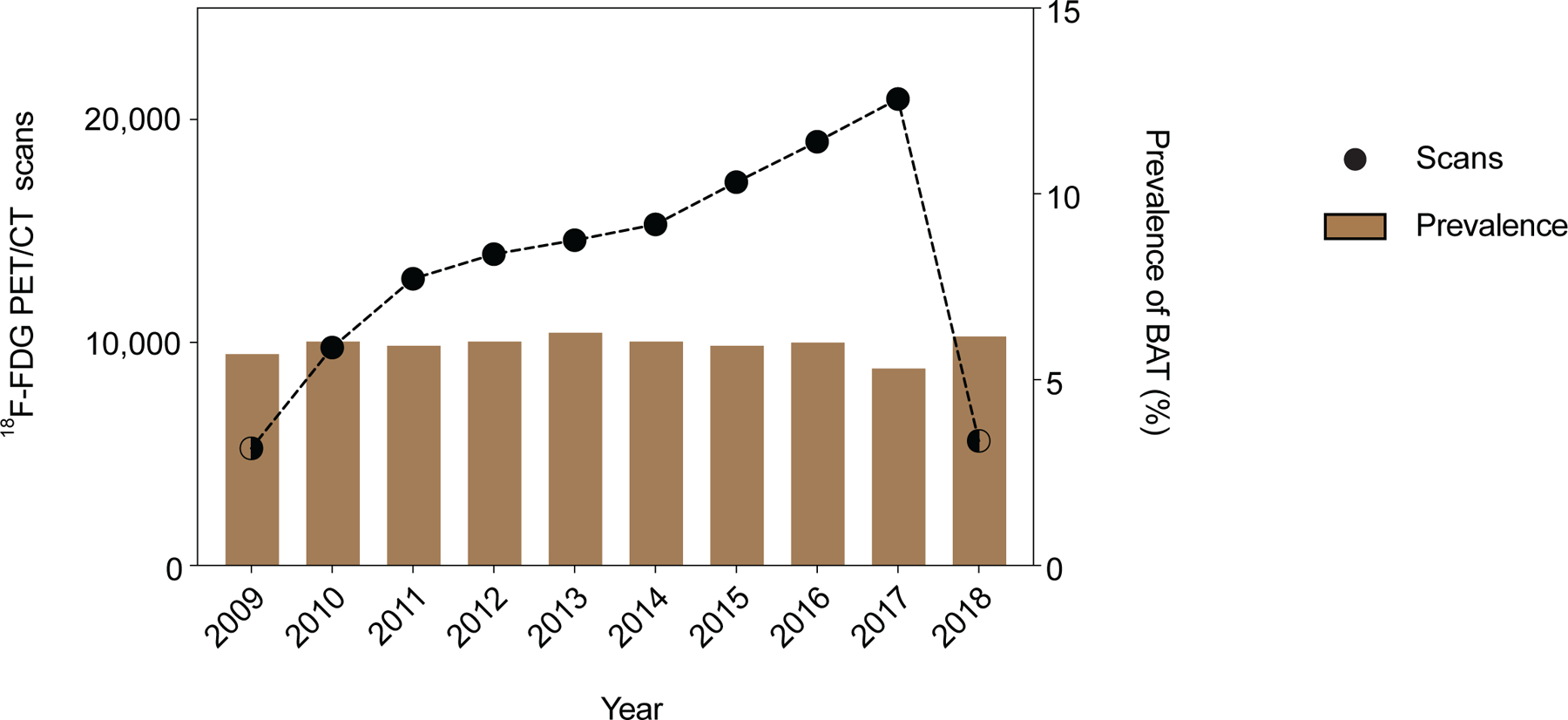
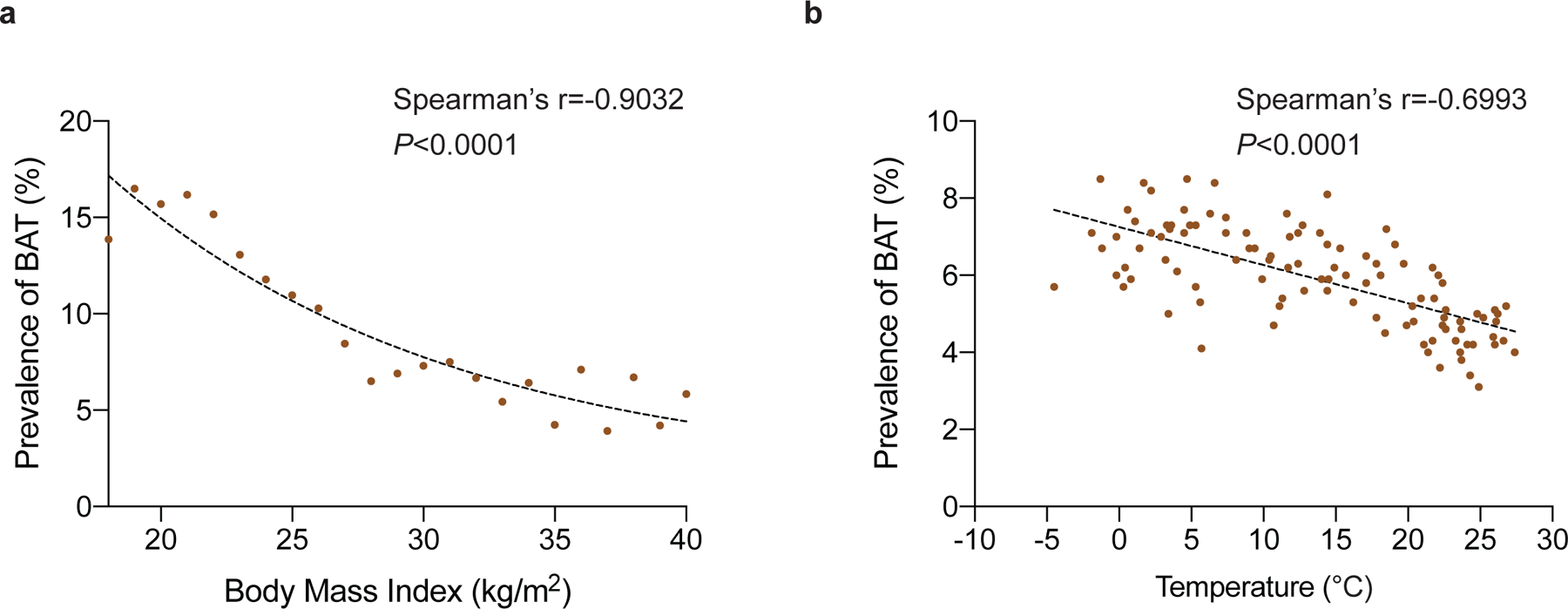
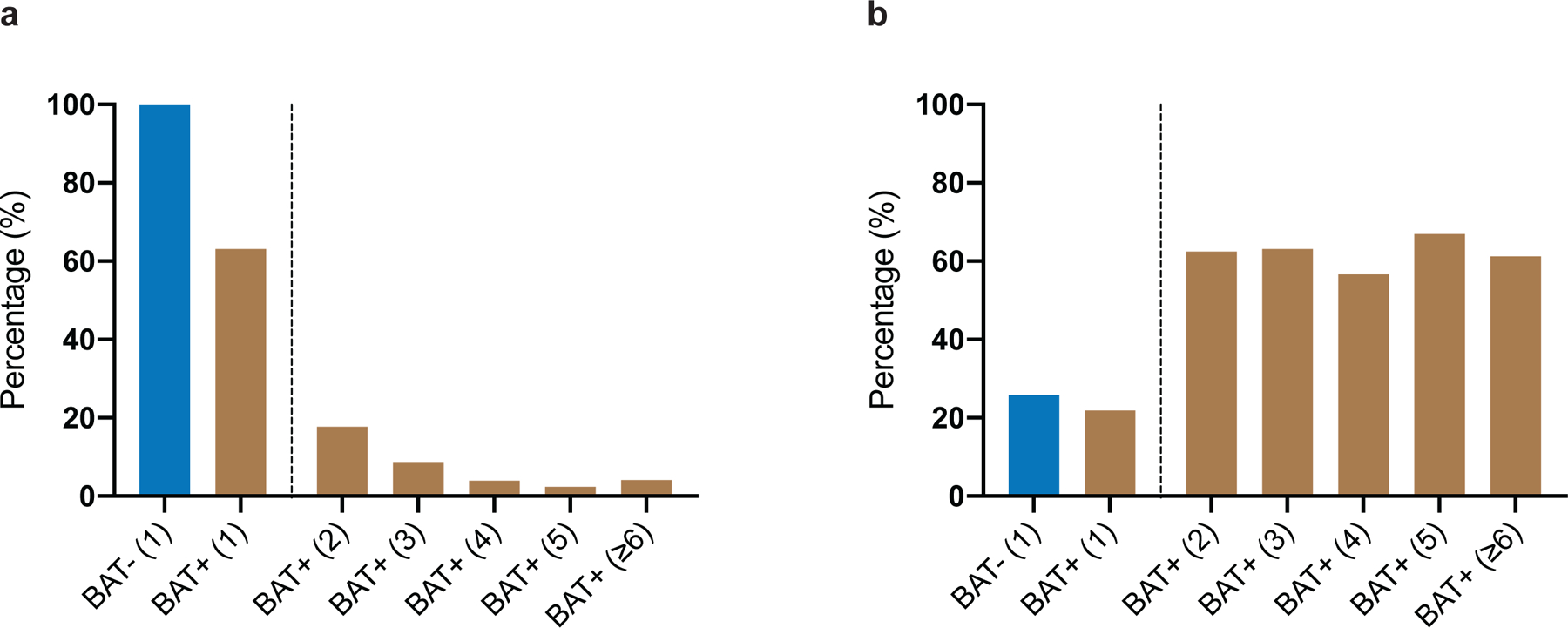
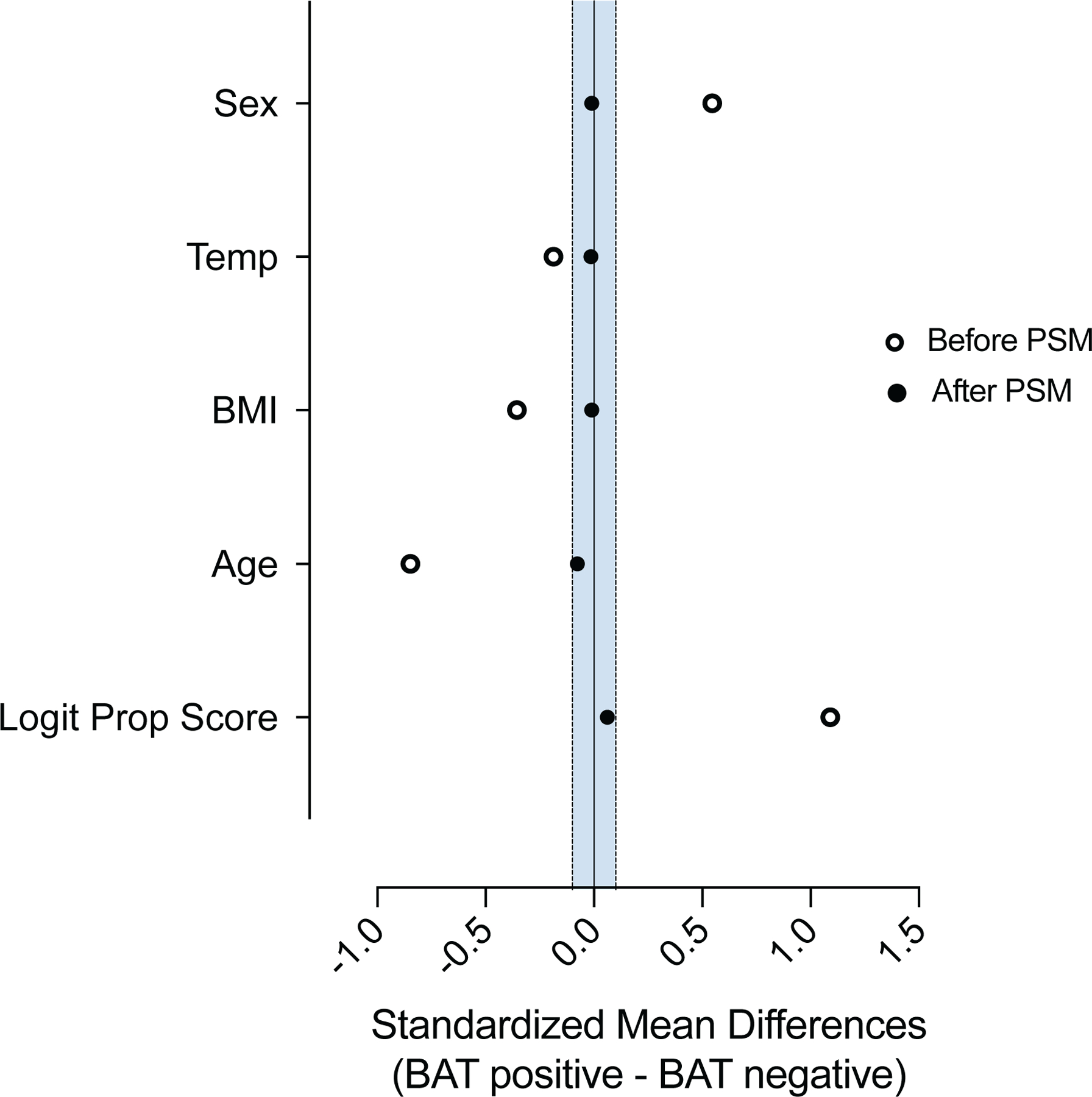
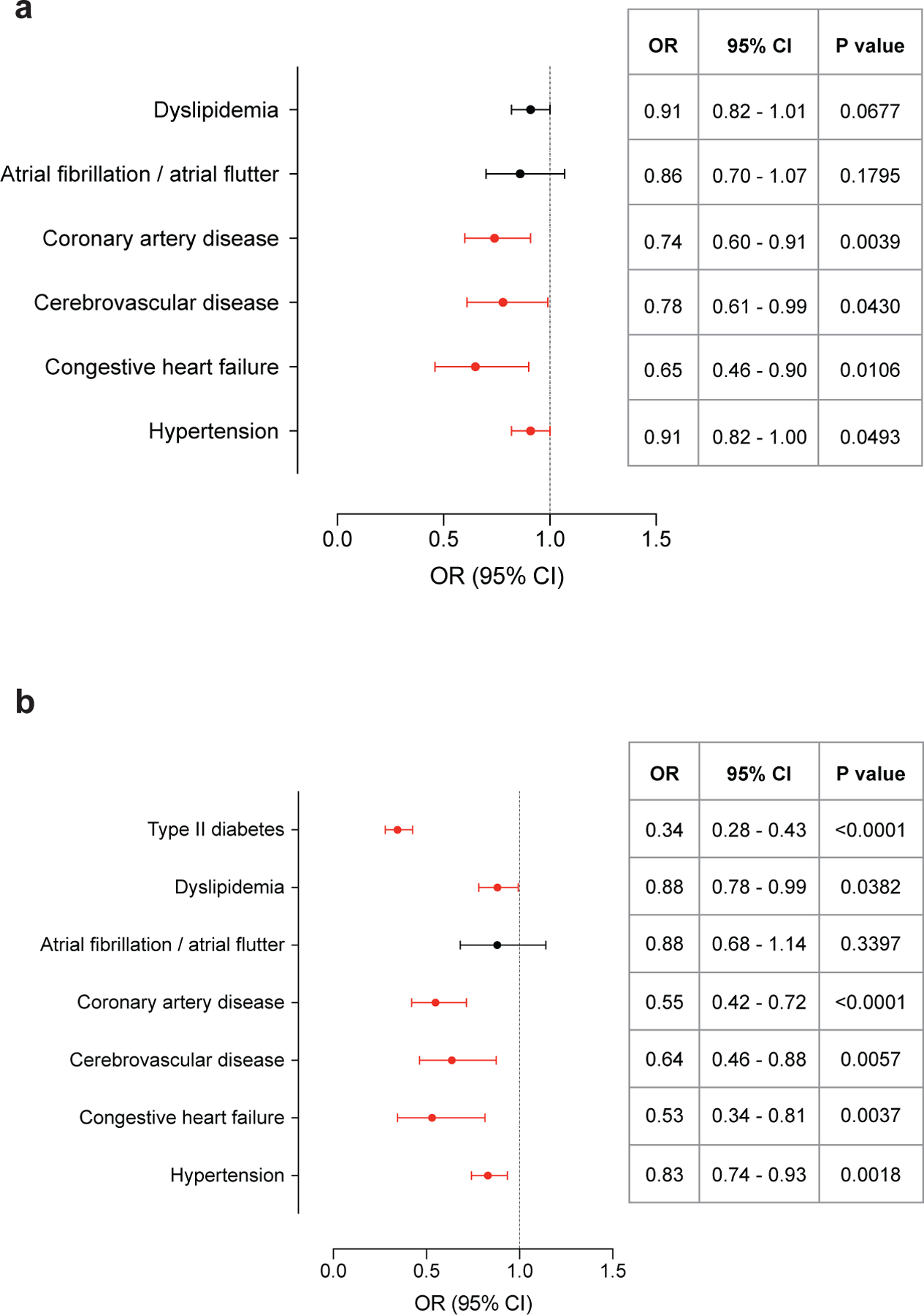
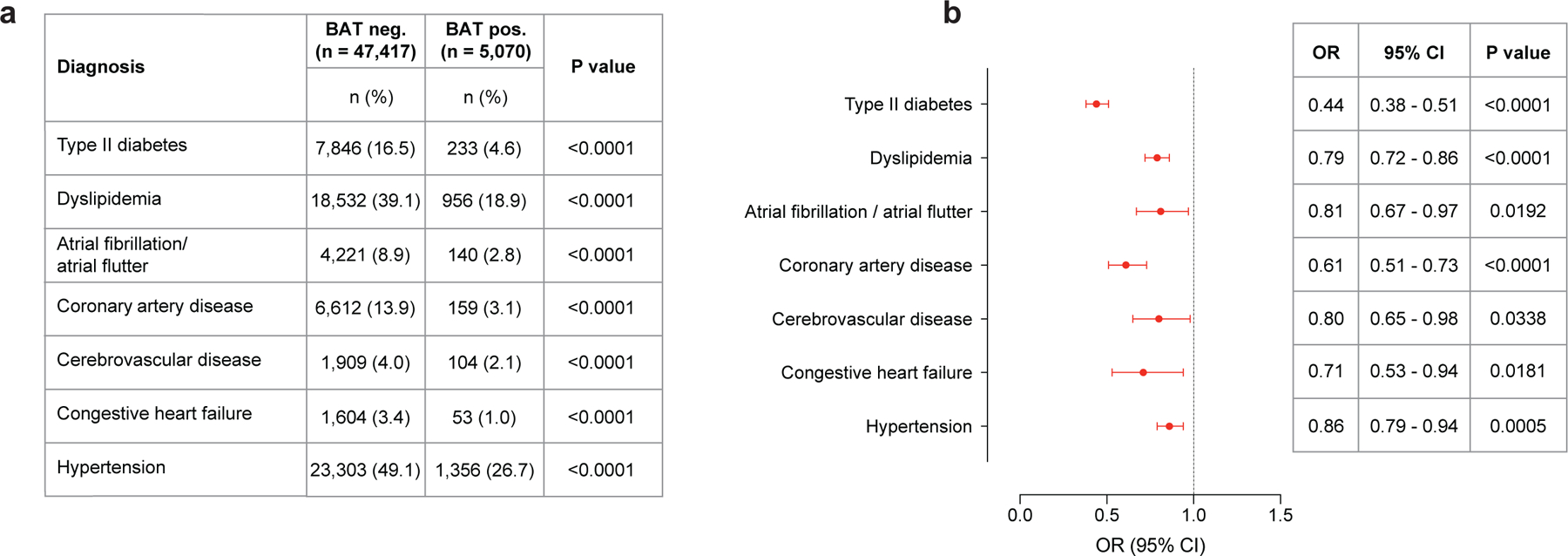
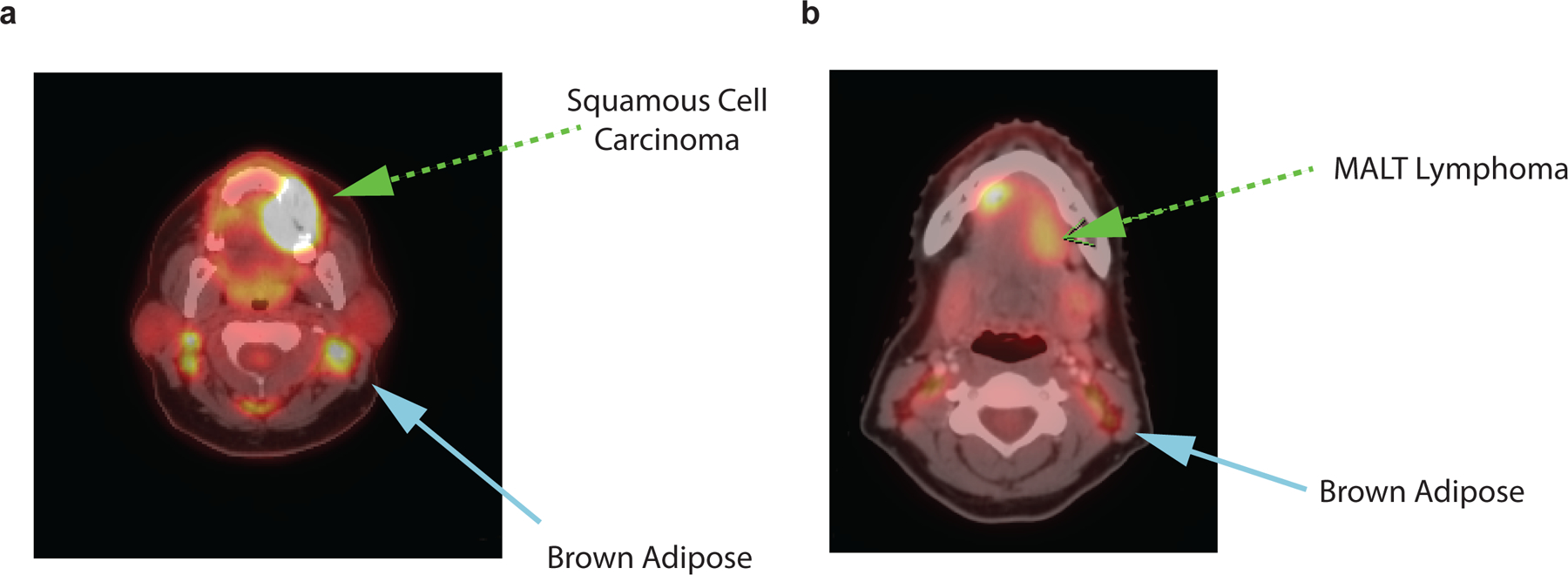
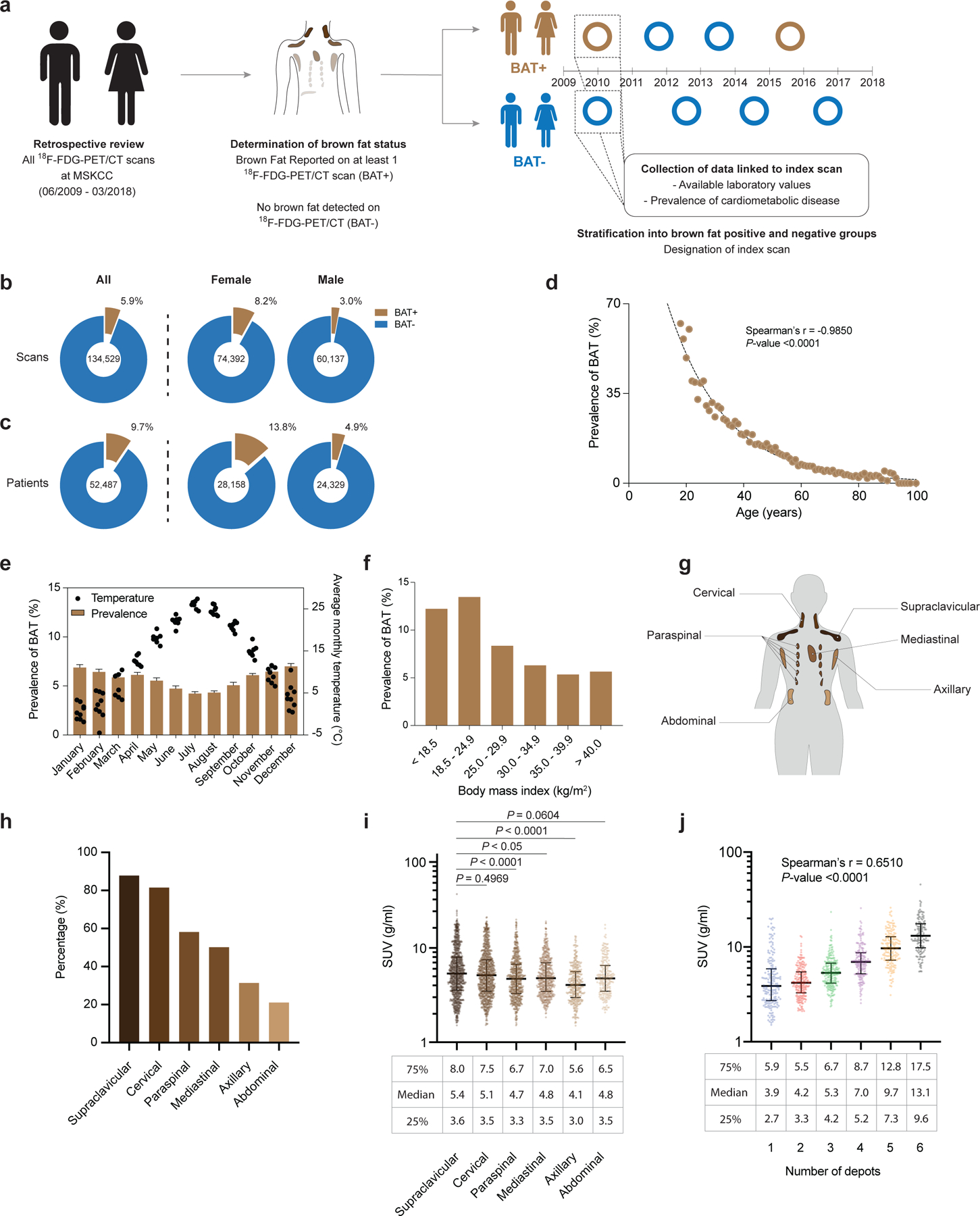
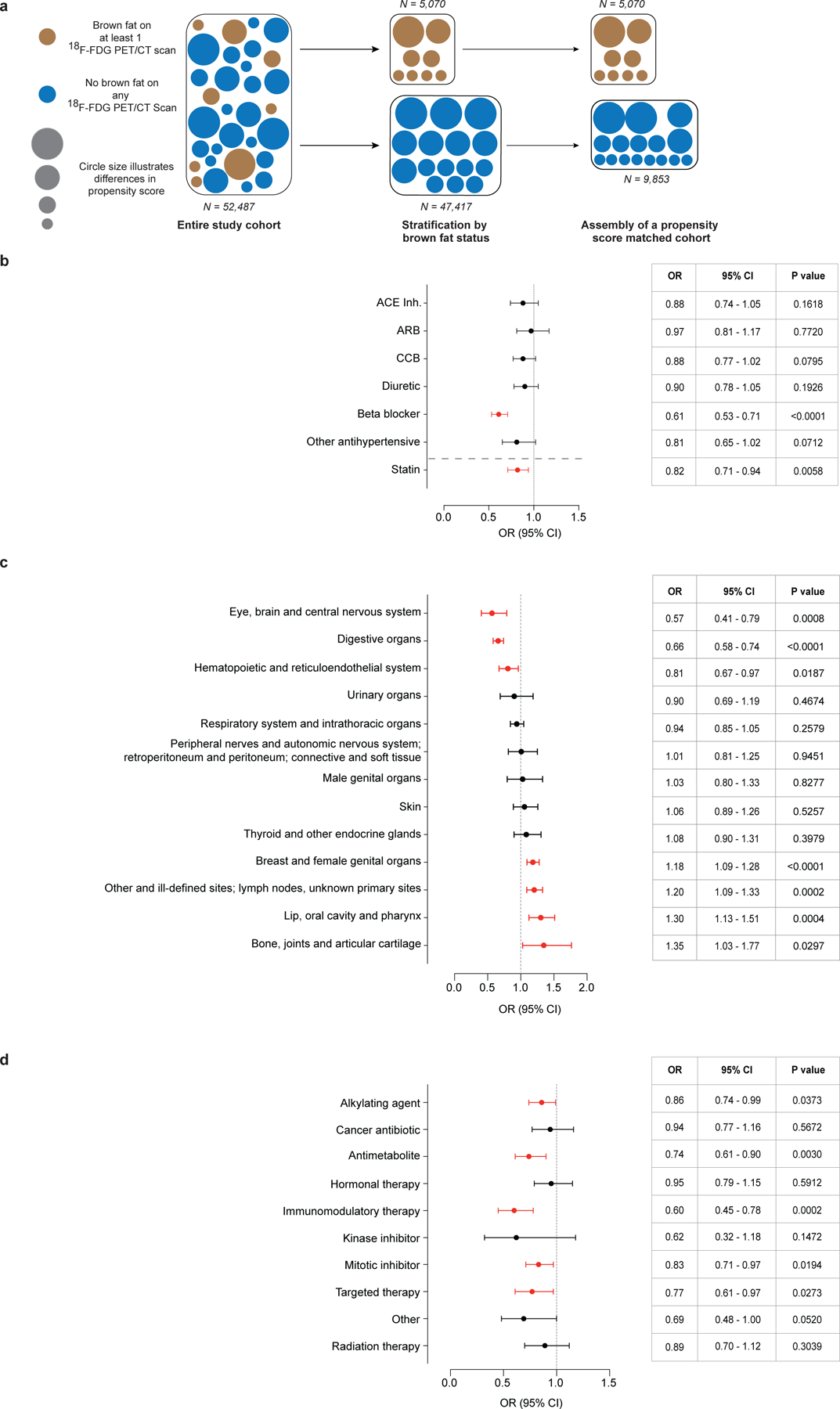
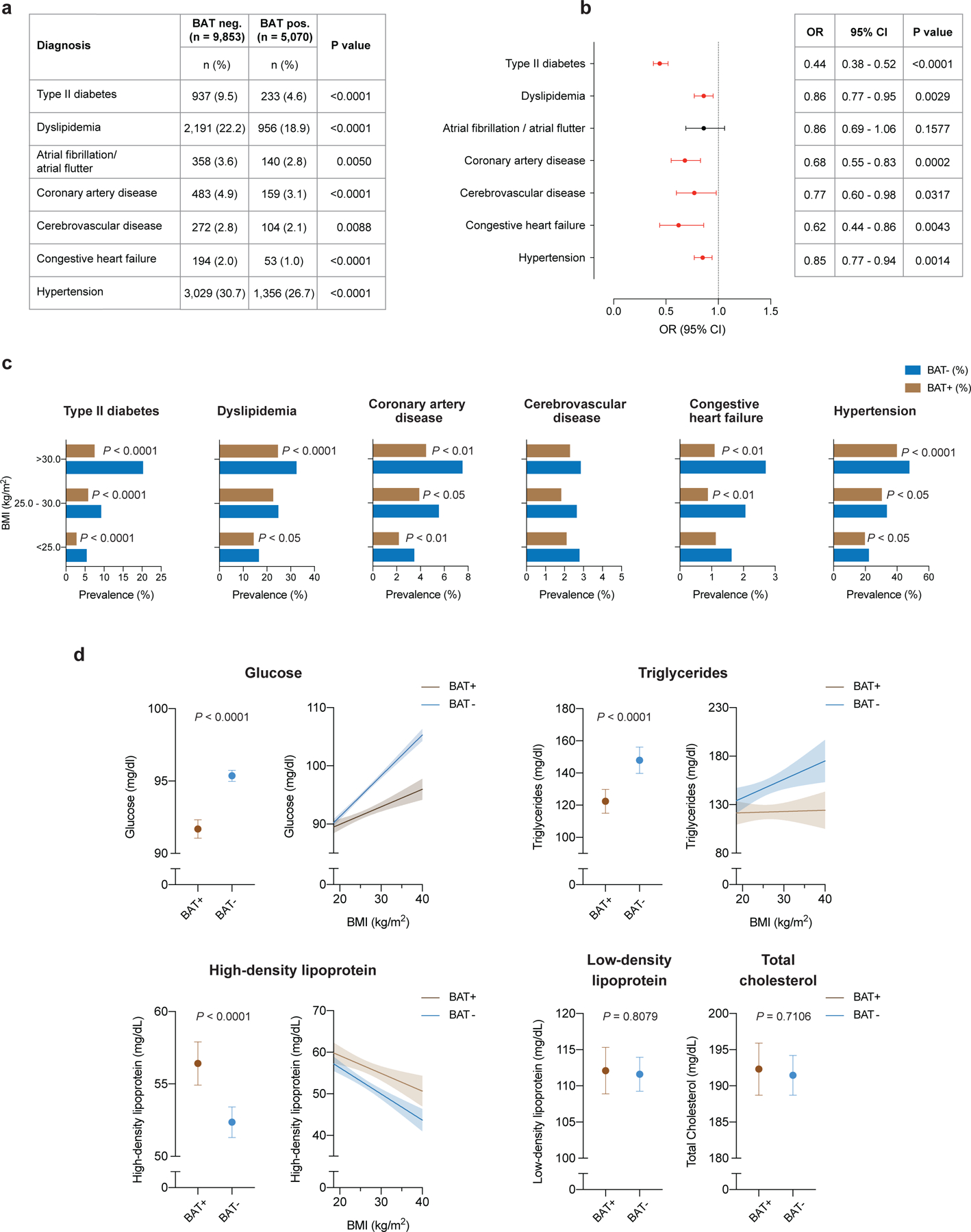
White fat stores excess energy, whereas brown and beige fat are thermogenic and dissipate energy as heat. Thermogenic adipose tissues markedly improve glucose and lipid homeostasis in mouse models, although the extent to which brown adipose tissue (BAT) influences metabolic and cardiovascular disease in humans is unclear1,2. Here we retrospectively categorized 134,529 18F-fluorodeoxyglucose positron emission tomography-computed tomography scans from 52,487 patients, by presence or absence of BAT, and used propensity score matching to assemble a study cohort. Scans in the study population were initially conducted for indications related to cancer diagnosis, treatment or surveillance, without previous stimulation. We report that individuals with BAT had lower prevalences of cardiometabolic diseases, and the presence of BAT was independently correlated with lower odds of type 2 diabetes, dyslipidemia, coronary artery disease, cerebrovascular disease, congestive heart failure and hypertension. These findings were supported by improved blood glucose, triglyceride and high-density lipoprotein values. The beneficial effects of BAT were more pronounced in individuals with overweight or obesity, indicating that BAT might play a role in mitigating the deleterious effects of obesity. Taken together, our findings highlight a potential role for BAT in promoting cardiometabolic health.
Conflict of interest statement
Competing Interest Statement
The authors declare no competing interests.
Figures
Comment in
-
Brown fat promotes cardiometabolic health.Nat Rev Cardiol. 2021 Apr;18(4):231. doi: 10.1038/s41569-021-00508-5. Nat Rev Cardiol. 2021. PMID: 33441974 No abstract available.
-
Human BAT linked with cardiometabolic health.Nat Rev Endocrinol. 2021 Mar;17(3):132. doi: 10.1038/s41574-021-00469-2. Nat Rev Endocrinol. 2021. PMID: 33462401 No abstract available.
References
-
- Bartelt A, et al. Brown adipose tissue activity controls triglyceride clearance. Nat. Med 17, 200–205 (2011). - PubMed
-
- Cohade C, Osman M, Pannu HK & Wahl RL Uptake in supraclavicular area fat (“USA-Fat”): Description on 18F-FDG PET/CT. J. Nucl. Med 44, 170–176 (2003). - PubMed
-
- van Marken Lichtenbelt WD, et al. Cold-activated brown adipose tissue in healthy men. N. Engl. J. Med 360, 1500–1508 (2009). - PubMed
-
- Virtanen KA, et al. Functional brown adipose tissue in healthy adults. N. Engl. J. Med 360, 1518–1525 (2009). - PubMed
References (method section)
-
- von Elm E, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Lancet 370, 1453–1457 (2007). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
