

Clinical Characteristics and Outcomes of COVID-19 Cohort Patients in Daegu Metropolitan City Outbreak in 2020
- PMID: 33398946
- PMCID: PMC7781854
- DOI: 10.3346/jkms.2021.36.e12
Clinical Characteristics and Outcomes of COVID-19 Cohort Patients in Daegu Metropolitan City Outbreak in 2020
Abstract
Background: A coronavirus disease 2019 (COVID-19) outbreak started in February 2020 and was controlled at the end of March 2020 in Daegu, the epicenter of the coronavirus outbreak in Korea. The aim of this study was to describe the clinical course and outcomes of patients with COVID-19 in Daegu.
Methods: In collaboration with Daegu Metropolitan City and Korean Center for Diseases Control, we conducted a retrospective, multicenter cohort study. Demographic, clinical, treatment, and laboratory data, including viral RNA detection, were obtained from the electronic medical records and cohort database and compared between survivors and non-survivors. We used univariate and multi-variable logistic regression methods and Cox regression model and performed Kaplan-Meier analysis to determine the risk factors associated with the 28-day mortality and release from isolation among the patients.
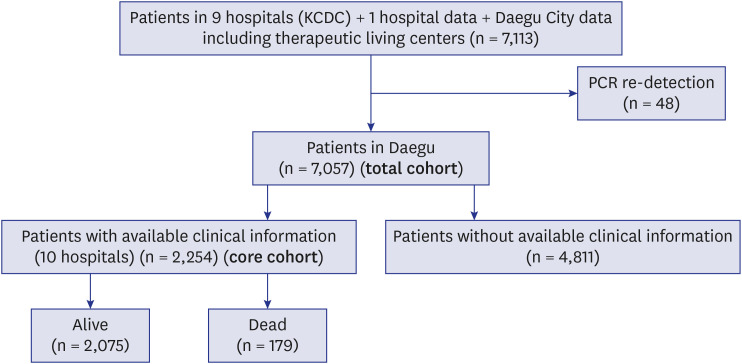
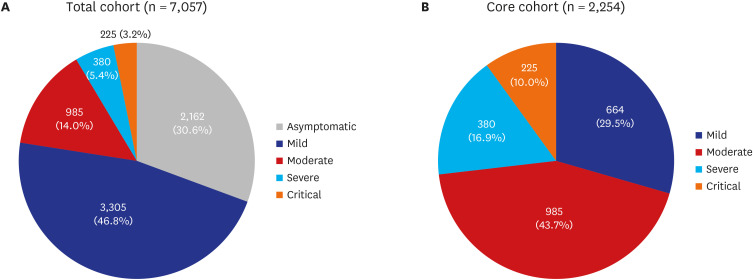
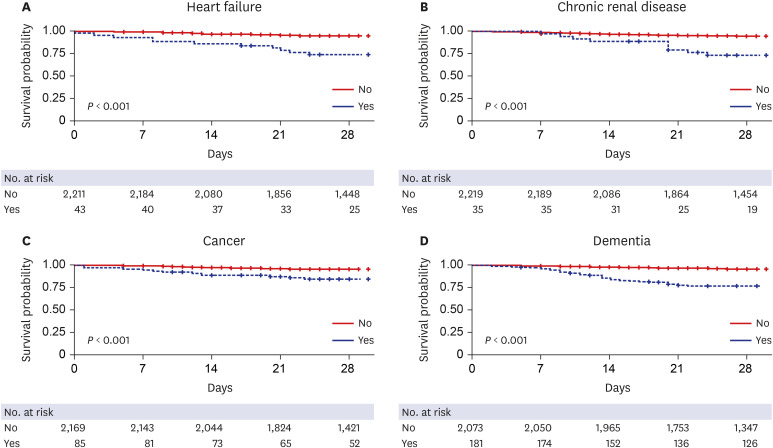
Results: In this study, 7,057 laboratory-confirmed patients with COVID-19 (total cohort) who had been diagnosed from February 18 to July 10, 2020 were included. Of the total cohort, 5,467 were asymptomatic to mild patients (77.4%) (asymptomatic 30.6% and mild 46.8%), 985 moderate (14.0%), 380 severe (5.4%), and 225 critical (3.2%). The mortality of the patients was 2.5% (179/7,057). The Cox regression hazard model for the patients with available clinical information (core cohort) (n = 2,254) showed the risk factors for 28-day mortality: age > 70 (hazard ratio [HR], 4.219, P = 0.002), need for O₂ supply at admission (HR, 2.995; P = 0.001), fever (> 37.5°C) (HR, 2.808; P = 0.001), diabetes (HR, 2.119; P = 0.008), cancer (HR, 3.043; P = 0.011), dementia (HR, 5.252; P = 0.008), neurological disease (HR, 2.084; P = 0.039), heart failure (HR, 3.234; P = 0.012), and hypertension (HR, 2.160; P = 0.017). The median duration for release from isolation was 33 days (interquartile range, 24.0-46.0) in survivors. The Cox proportional hazard model for the long duration of isolation included severity, age > 70, and dementia.
Conclusion: Overall, asymptomatic to mild patients were approximately 77% of the total cohort (asymptomatic, 30.6%). The case fatality rate was 2.5%. Risk factors, including older age, need for O₂ supply, dementia, and neurological disorder at admission, could help clinicians to identify COVID-19 patients with poor prognosis at an early stage.
Keywords: COVID-19; Case Fatality Rate; Mortality; Outbreak; Outcome.
© 2021 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Kim JH, An AR, Min PK, Bitton A, Gawande AA. How South Korea responded to the COVID-19 outbreak in Daegu. NEJM Catal Innov Care Deliv. 2020;1(4):1–14.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
