

Longitudinal characterisation of haematological and biochemical parameters in cancer patients prior to and during COVID-19 reveals features associated with outcome
- PMID: 33399072
- PMCID: PMC7808077
- DOI: 10.1016/j.esmoop.2020.100005
Longitudinal characterisation of haematological and biochemical parameters in cancer patients prior to and during COVID-19 reveals features associated with outcome
Erratum in
-
Erratum to 'Longitudinal characterisation of haematological and biochemical parameters in cancer patients prior to and during COVID-19 reveals features associated with outcome': [ESMO Open Volume 6, Issue 1, February 2021, 100005].ESMO Open. 2021 Apr;6(2):100056. doi: 10.1016/j.esmoop.2021.100056. Epub 2021 Jan 28. ESMO Open. 2021. PMID: 33545518 Free PMC article. No abstract available.
Abstract
Background: Cancer patients are at increased risk of death from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Cancer and its treatment affect many haematological and biochemical parameters, therefore we analysed these prior to and during coronavirus disease 2019 (COVID-19) and correlated them with outcome.
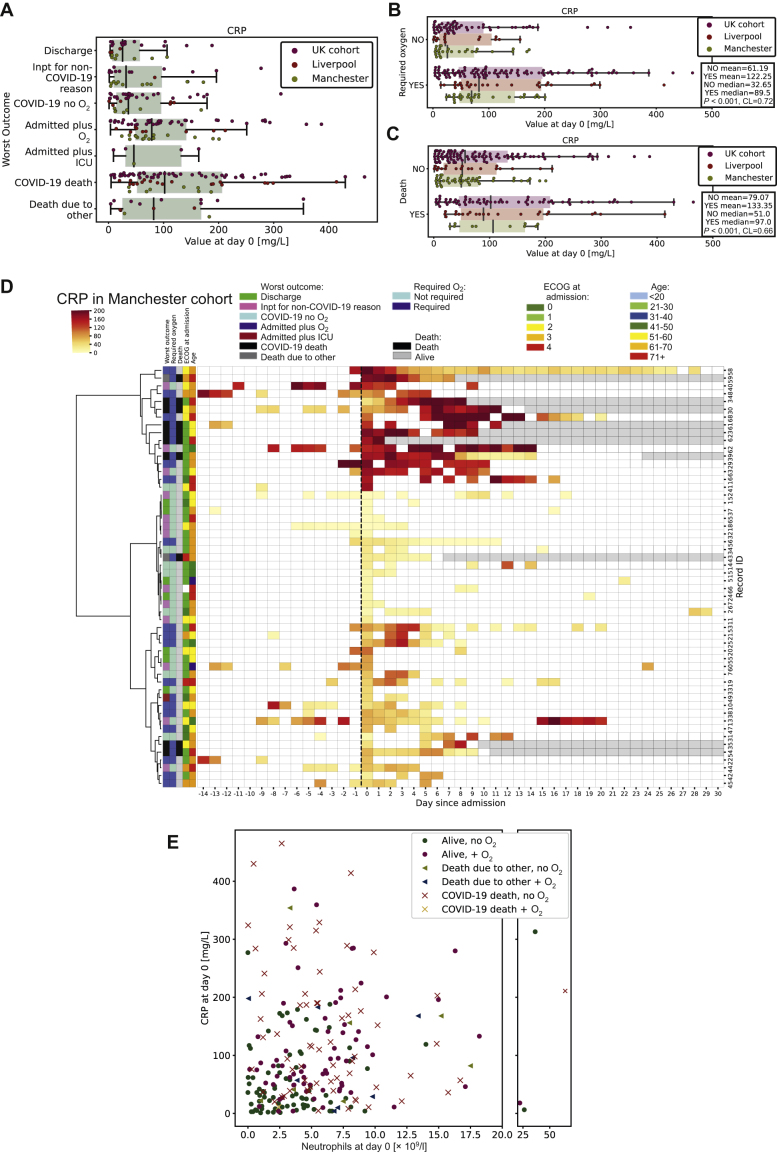
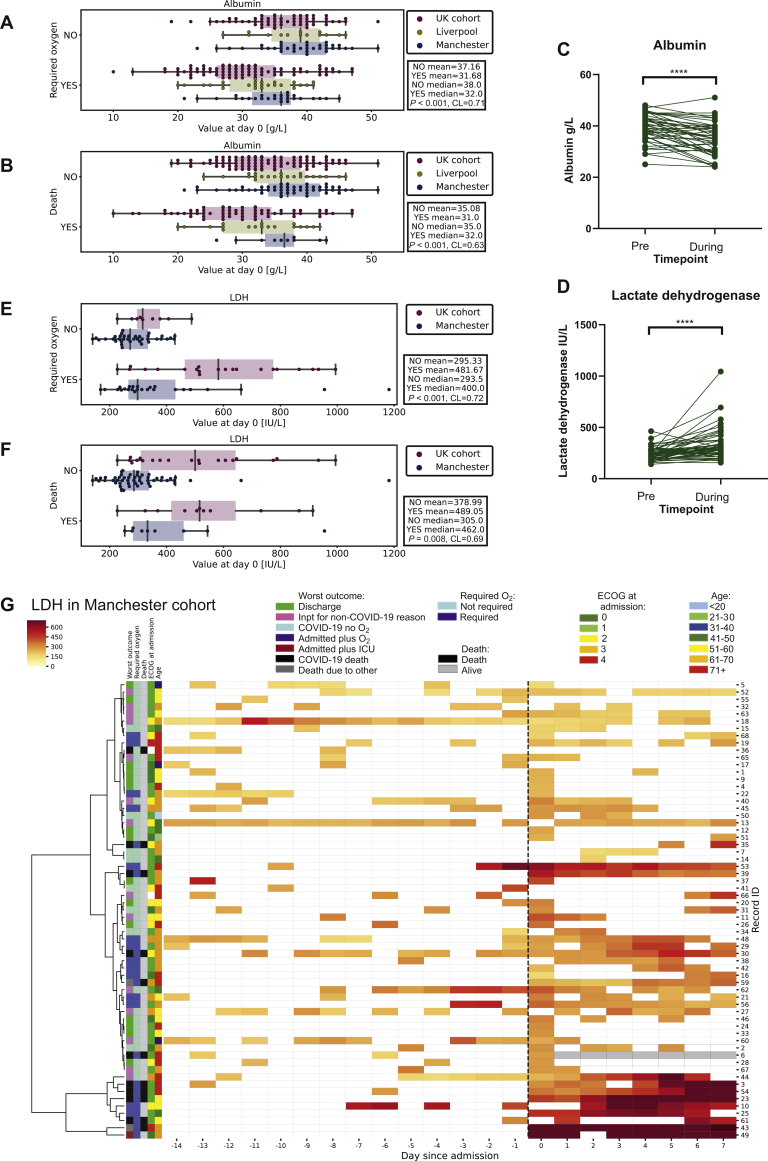
Patients and methods: Consecutive patients with cancer testing positive for SARS-CoV-2 in centres throughout the United Kingdom were identified and entered into a database following local governance approval. Clinical and longitudinal laboratory data were extracted from patient records. Data were analysed using Mann-Whitney U test, Fisher's exact test, Wilcoxon signed rank test, logistic regression, or linear regression for outcomes. Hierarchical clustering of heatmaps was performed using Ward's method.
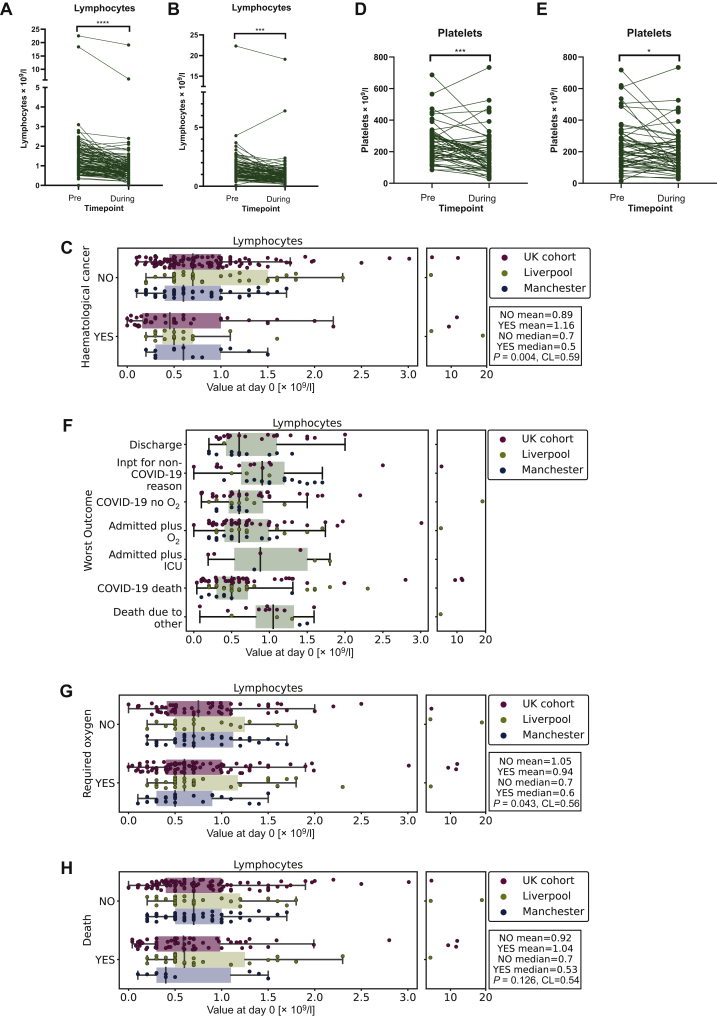
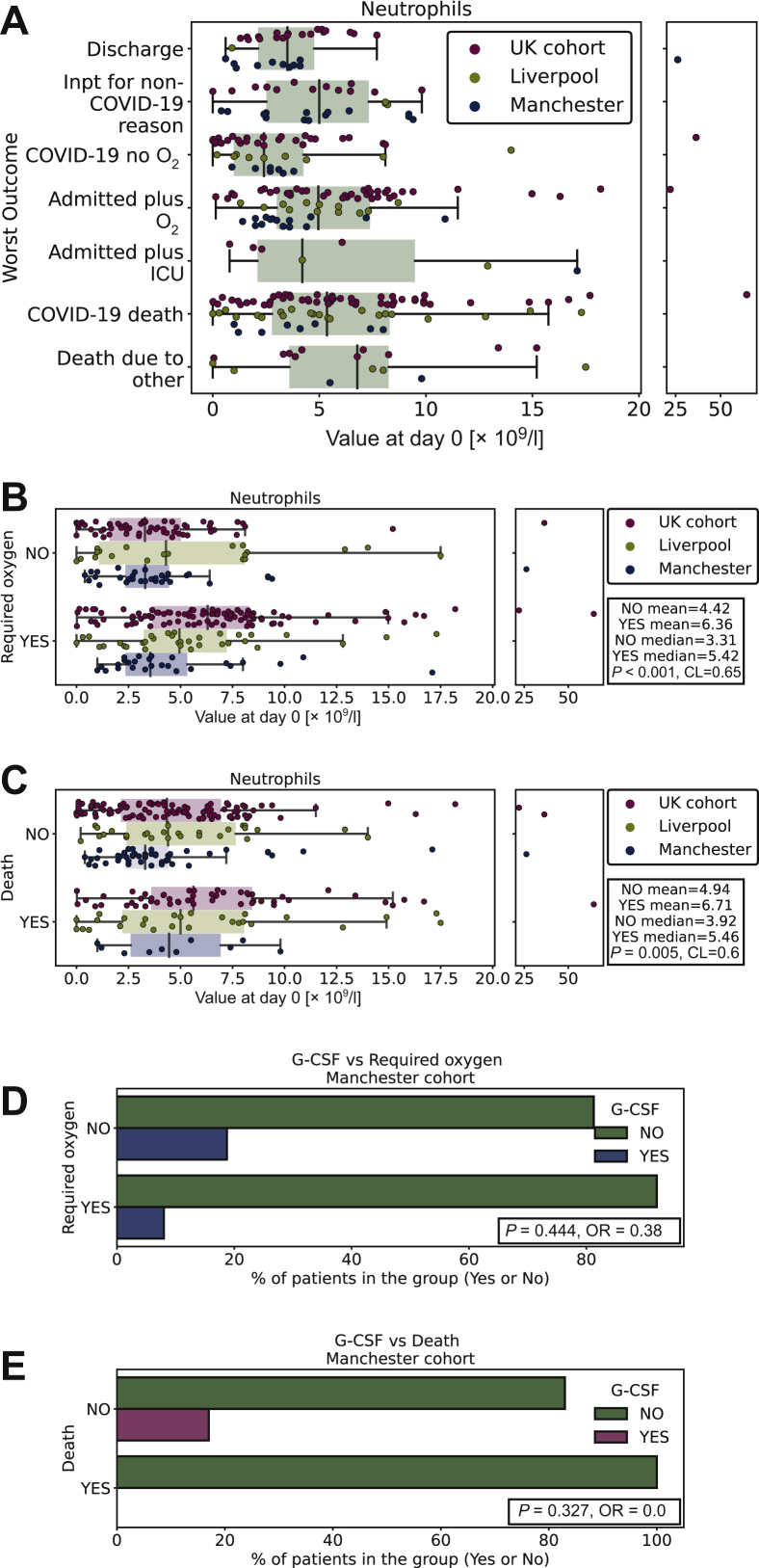
Results: In total, 302 patients were included in three cohorts: Manchester (n = 67), Liverpool (n = 62), and UK (n = 173). In the entire cohort (N = 302), median age was 69 (range 19-93 years), including 163 males and 139 females; of these, 216 were diagnosed with a solid tumour and 86 with a haematological cancer. Preinfection lymphopaenia, neutropaenia and lactate dehydrogenase (LDH) were not associated with oxygen requirement (O2) or death. Lymphocyte count (P < 0.001), platelet count (P = 0.03), LDH (P < 0.0001) and albumin (P < 0.0001) significantly changed from preinfection to during infection. High rather than low neutrophils at day 0 (P = 0.007), higher maximal neutrophils during COVID-19 (P = 0.026) and higher neutrophil-to-lymphocyte ratio (NLR; P = 0.01) were associated with death. In multivariable analysis, age (P = 0.002), haematological cancer (P = 0.034), C-reactive protein (P = 0.004), NLR (P = 0.036) and albumin (P = 0.02) at day 0 were significant predictors of death. In the Manchester/Liverpool cohort 30 patients have restarted therapy following COVID-19, with no additional complications requiring readmission.
Conclusion: Preinfection biochemical/haematological parameters were not associated with worse outcome in cancer patients. Restarting treatment following COVID-19 was not associated with additional complications. Neutropaenia due to cancer/treatment is not associated with COVID-19 mortality. Cancer therapy, particularly in patients with solid tumours, need not be delayed or omitted due to concerns that treatment itself increases COVID-19 severity.
Keywords: COVID-19; SARS-CoV-2; cancer.
Copyright © 2020 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure RJL speaker fees BMS and Astrazeneca, MR honoraria from Astellas Pharma, speaker fees MSD and Servier. CW consultancy and speaker fees Pfizer, Amgen, Novartis, AA conference fee Merck, spouse shares in Astrazeneca. TR financial support to attend educational workshops from Amgen and Daiichi-Sankyo. JT is now working at Astra Zeneca. CD, outside of this scope of work, has received research funding from AstraZeneca, Astex Pharmaceuticals, Bioven, Amgen, Carrick Therapeutics, Merck AG, Taiho Oncology, Clearbridge Biomedics, Angle PLC, Menarini Diagnostics, GSK, Bayer, Boehringer Ingelheim, Roche, BMS, Novartis, Celgene, Thermofisher. CD is on advisory boards for, and has received consultancy fees/honoraria from, AstraZeneca, Biocartis and Merck KGaA. The remaining authors have no conflicts of interest to declare.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
