

Robotic Complete Mesocolic Excision (CME) is a safe and feasible option for right colonic cancers: short and midterm results from a single-centre experience
- PMID: 33399993
- PMCID: PMC8599208
- DOI: 10.1007/s00464-020-08194-z
Robotic Complete Mesocolic Excision (CME) is a safe and feasible option for right colonic cancers: short and midterm results from a single-centre experience
Abstract
Background: Complete mesocolic excision (CME) for right colon cancers has traditionally been an open procedure. Surgical adoption of minimal access CME remains limited due to the technical challenges, training gaps and lack of level-1 data for proven benefits. Currently there is limited published data regarding the clinical results with the use of robotic CME surgery. Aim To report our experience, results and techniques, highlighting a clinical and oncological results and midterm oncological outcomes for robotic CME.
Aim: To report our experience, results and techniques, highlighting a clinical and oncological results and midterm oncological outcomes for robotic CME.
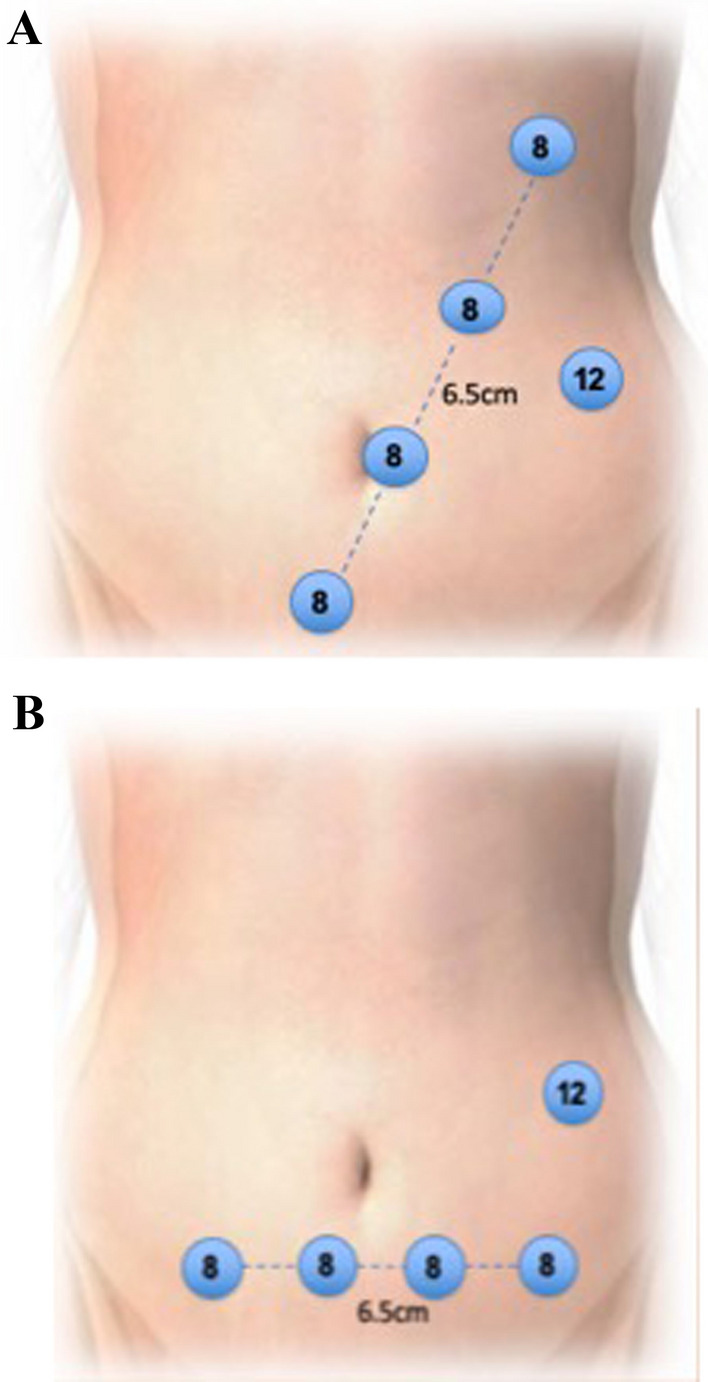
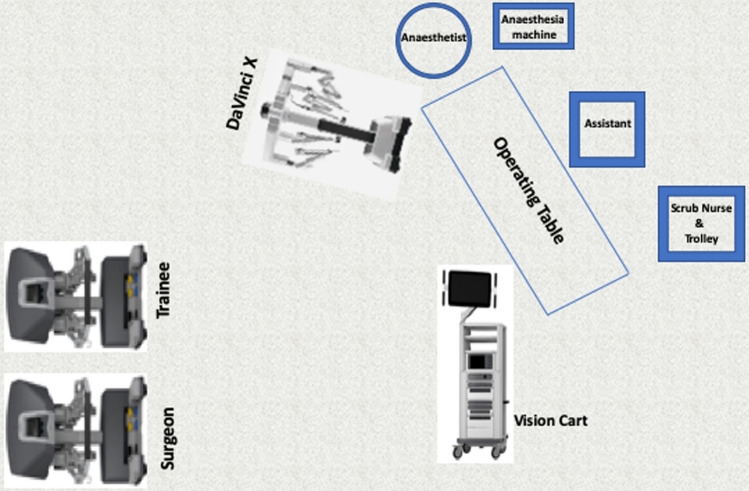
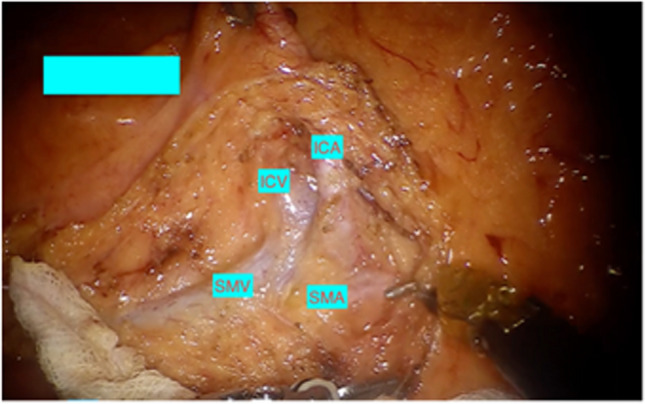
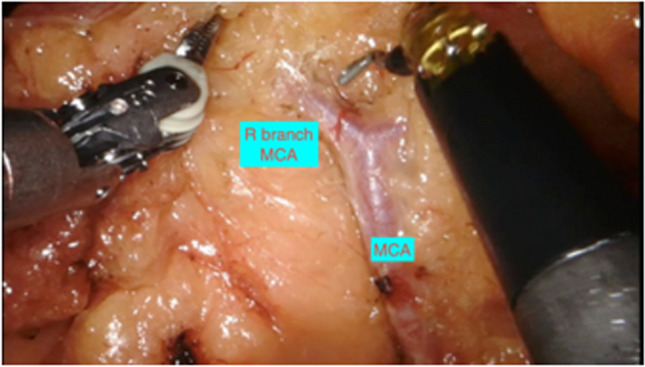
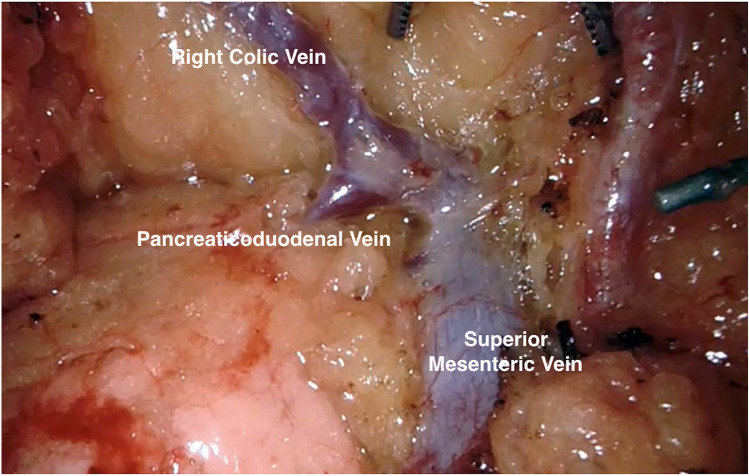
Methods: All patients undergoing standardised robotic CME technique with SMV first approach between January 2015 and September 2019 were included in this retrospective review of a prospectively collected database. Patient demographics, operative data and clinical and oncological outcomes were recorded.
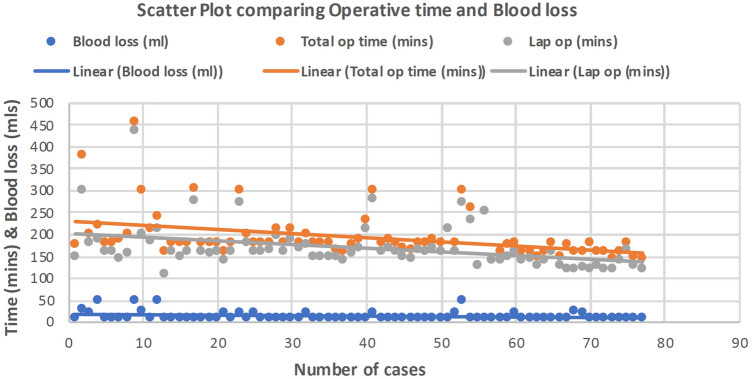
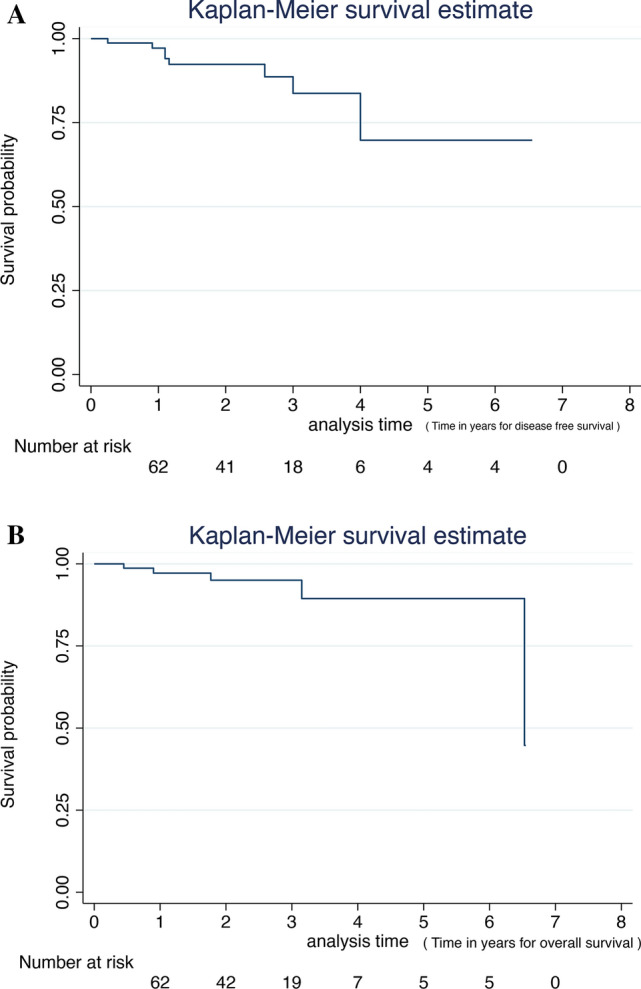
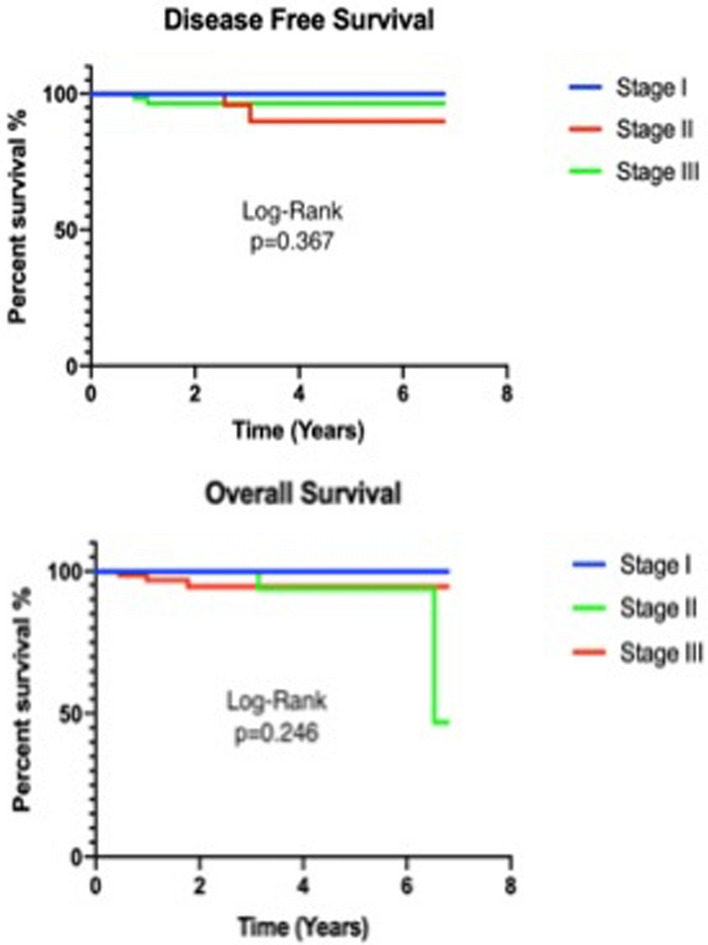
Results: Seventy-seven robotic CME resections for right colonic cancers were performed over a 4-year period. Median operative time was 180 (128-454) min and perioperative blood loss was 10 (10-50) ml. There were 25 patients who had previous abdominal surgery. Median postoperative hospital stay was 5 (3-18) days. There was no conversion to open surgery in this series. Median lymph node count was 30 (10-60). Three (4%) patients had R1 resection. There was one (1%) local recurrence in stage III disease and 4(5%) distal recurrence in stage II and stage III. There was no 30- or 90-day mortality. Three-year disease-free survival was 100%, 91.7% and 92% for stages I, II and III, respectively. Overall survival was 94%.
Conclusions: Robotic CME is feasible, effective and safe. Good oncological results and improved survival are seen in this cohort of patients with a standardised approach to robotic CME.
Keywords: Complete Mesocolic Excision; Right colon cancer; Robotic surgery; Techniques.
© 2021. The Author(s).
Conflict of interest statement
Jim Khan: Trainer and proctor with Intuitive Surgical and Johnson & Johnson. Najaf N. Siddiqi, Sam Stefan, Ravish Jootun, and Gerald David have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Colon Cancer Laparoscopic or Open Resection Study Group, Buunen M, Veldkamp R, Hop WCJ, Kuhry E, Jeekel J, Haglind E, Påhlman L, Cuesta MA, Msika S, Morino M, Lacy A, Bonjer HJ (2009) Survival after laparoscopic surgery versus open surgery for colon cancer: long-term outcome of a randomised clinical trial. Lancet Oncol 10:44–52. 10.1016/S1470-2045(08)70310-3 - PubMed
-
- Fleshman J, Sargent DJ, Green E, Anvari M, Stryker SJ, Beart RW, Hellinger M, Flanagan R, Peters W, Nelson H, Clinical Outcomes of Surgical Therapy Study Group (2007) Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg 246:655–62; discussion 662-4. 10.1097/sla.0b013e318155a762 - PubMed
-
- Cecil TD, Sexton R, Moran BJ, Heald RJ (2004) Total mesorectal excision results in low local recurrence rates in lymph node-positive rectal cancer. Dis Colon Rectum 47:1145–9; discussion 1149-50. 10.1007/s10350-004-0086-6 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
