

The Duration, Dynamics, and Determinants of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Antibody Responses in Individual Healthcare Workers
- PMID: 33400782
- PMCID: PMC7929225
- DOI: 10.1093/cid/ciab004
The Duration, Dynamics, and Determinants of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Antibody Responses in Individual Healthcare Workers
Abstract
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) immunoglobulin G (IgG) antibody measurements can be used to estimate the proportion of a population exposed or infected and may be informative about the risk of future infection. Previous estimates of the duration of antibody responses vary.
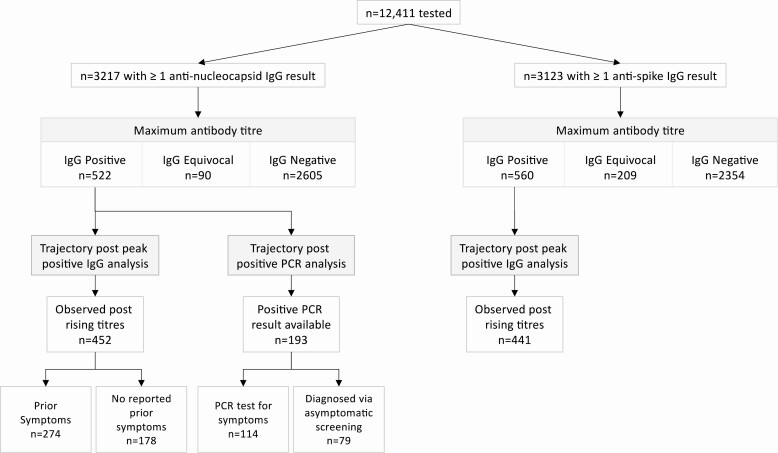
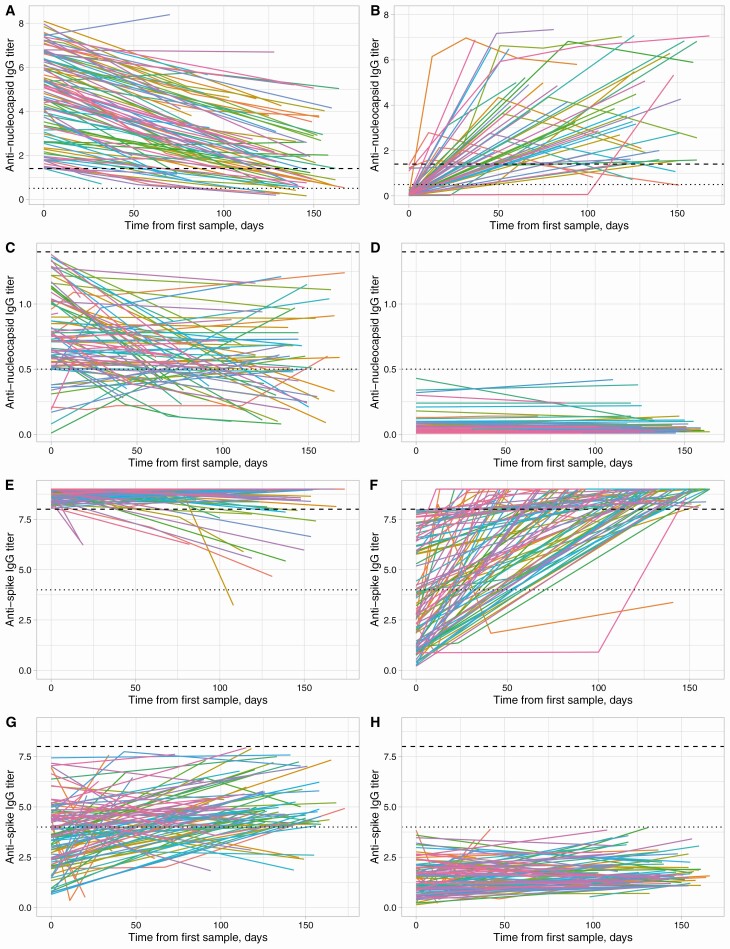
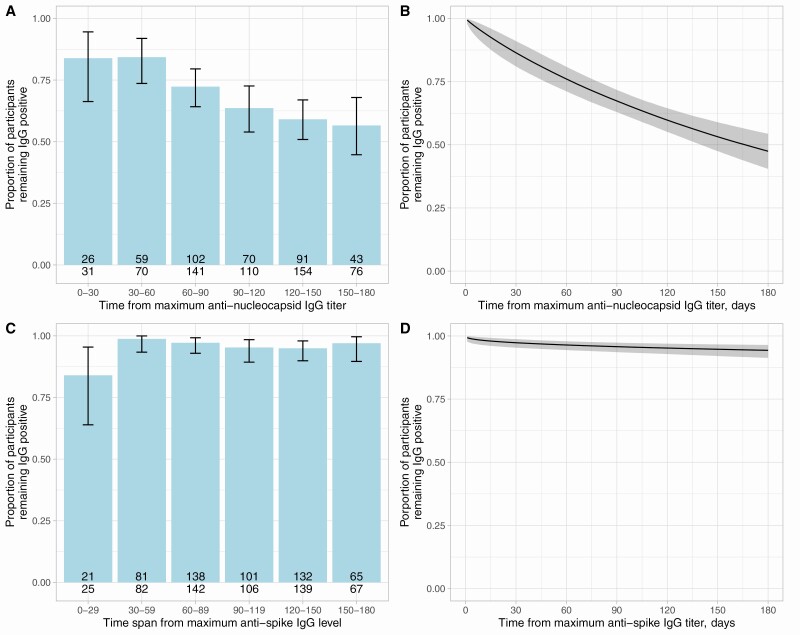
Methods: We present 6 months of data from a longitudinal seroprevalence study of 3276 UK healthcare workers (HCWs). Serial measurements of SARS-CoV-2 anti-nucleocapsid and anti-spike IgG were obtained. Interval censored survival analysis was used to investigate the duration of detectable responses. Additionally, Bayesian mixed linear models were used to investigate anti-nucleocapsid waning.
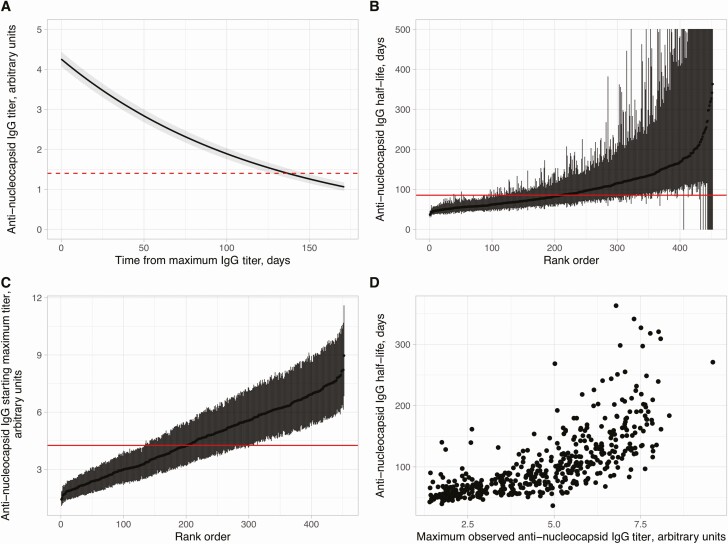
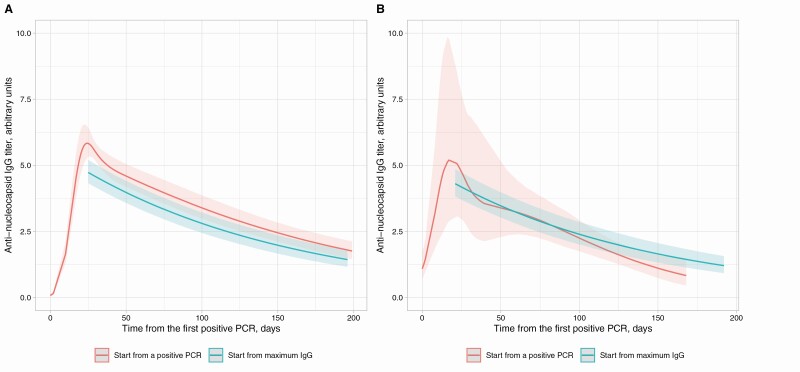
Results: Anti-spike IgG levels remained stably detected after a positive result, for example, in 94% (95% credibility interval [CrI] 91-96%) of HCWs at 180 days. Anti-nucleocapsid IgG levels rose to a peak at 24 (95% CrI 19-31) days post first polymerase chain reaction (PCR)-positive test, before beginning to fall. Considering 452 anti-nucleocapsid seropositive HCWs over a median of 121 days from their maximum positive IgG titer, the mean estimated antibody half-life was 85 (95% CrI 81-90) days. Higher maximum observed anti-nucleocapsid titers were associated with longer estimated antibody half-lives. Increasing age, Asian ethnicity, and prior self-reported symptoms were independently associated with higher maximum anti-nucleocapsid levels and increasing age and a positive PCR test undertaken for symptoms with longer anti-nucleocapsid half-lives.
Conclusions: SARS-CoV-2 anti-nucleocapsid antibodies wane within months and fall faster in younger adults and those without symptoms. However, anti-spike IgG remains stably detected. Ongoing longitudinal studies are required to track the long-term duration of antibody levels and their association with immunity to SARS-CoV-2 reinfection.
Keywords: COVID-19; SARS-CoV-2; antibody; longitudinal; serology.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
Comment in
-
Protection of Healthcare Workers Against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Reinfection.Clin Infect Dis. 2021 Oct 5;73(7):1323-1324. doi: 10.1093/cid/ciab069. Clin Infect Dis. 2021. PMID: 33503228 Free PMC article. No abstract available.
-
Estimated Half-Life of SARS-CoV-2 Anti-Spike Antibodies More Than Double the Half-Life of Anti-nucleocapsid Antibodies in Healthcare Workers.Clin Infect Dis. 2021 Dec 16;73(12):2366-2368. doi: 10.1093/cid/ciab219. Clin Infect Dis. 2021. PMID: 33693643 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
