

Proton and Heavy Particle Intracranial Radiosurgery
- PMID: 33401613
- PMCID: PMC7823941
- DOI: 10.3390/biomedicines9010031
Proton and Heavy Particle Intracranial Radiosurgery
Abstract
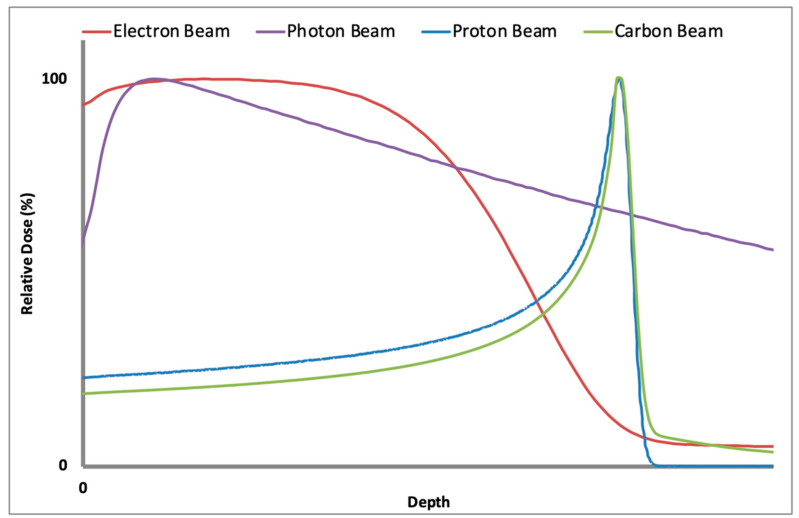
Stereotactic radiosurgery (SRS) involves the delivery of a highly conformal ablative dose of radiation to both benign and malignant targets. This has traditionally been accomplished in a single fraction; however, fractionated approaches involving five or fewer treatments have been delivered for larger lesions, as well as lesions in close proximity to radiosensitive structures. The clinical utilization of SRS has overwhelmingly involved photon-based sources via dedicated radiosurgery platforms (e.g., Gamma Knife® and Cyberknife®) or specialized linear accelerators. While photon-based methods have been shown to be highly effective, advancements are sought for improved dose precision, treatment duration, and radiobiologic effect, among others, particularly in the setting of repeat irradiation. Particle-based techniques (e.g., protons and carbon ions) may improve many of these shortcomings. Specifically, the presence of a Bragg Peak with particle therapy at target depth allows for marked minimization of distal dose delivery, thus mitigating the risk of toxicity to organs at risk. Carbon ions also exhibit a higher linear energy transfer than photons and protons, allowing for greater relative biological effectiveness. While the data are limited, utilization of proton radiosurgery in the setting of brain metastases has been shown to demonstrate 1-year local control rates >90%, which are comparable to that of photon-based radiosurgery. Prospective studies are needed to further validate the safety and efficacy of this treatment modality. We aim to provide a comprehensive overview of clinical evidence in the use of particle therapy-based radiosurgery.
Keywords: ablative; arteriovenous malformation; carbon; particle; proton; radiation oncology; radiation therapy; radiosurgery; stereotactic; tumor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand. 1951;102:316–319. - PubMed
-
- Lehrer E.J., Snyder M.H., Desai B., Li C.E., Narayan A., Trifiletti D.M., Schlesinger D., Sheehan J.P. Clinical and radiographic adverse events after Gamma Knife radiosurgery for brainstem lesions: A dosimetric analysis. Radiother. Oncol. 2020;147:200–209. doi: 10.1016/j.radonc.2020.05.010. - DOI - PubMed
-
- Minniti G., Esposito V., Clarke E., Scaringi C., Lanzetta G., Salvati M., Raco A., Bozzao A., Enrici R.M. Multidose stereotactic radiosurgery (9 Gy × 3) of the postoperative resection cavity for treatment of large brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 2013;86:623–629. doi: 10.1016/j.ijrobp.2013.03.037. - DOI - PubMed
-
- Minniti G., Scaringi C., Paolini S., Lanzetta G., Romano A., Cicone F., Osti M., Enrici R.M., Esposito V. Single-Fraction Versus Multifraction (3 × 9 Gy) Stereotactic Radiosurgery for Large (>2 cm) Brain Metastases: A Comparative Analysis of Local Control and Risk of Radiation-Induced Brain Necrosis. Int. J. Radiat. Oncol. Biol. Phys. 2016;95:1142–1148. doi: 10.1016/j.ijrobp.2016.03.013. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
