

Subaxial Cervical Spine Injuries: WFNS Spine Committee Recommendations
- PMID: 33401854
- PMCID: PMC7788423
- DOI: 10.14245/ns.2040368.184
Subaxial Cervical Spine Injuries: WFNS Spine Committee Recommendations
Abstract
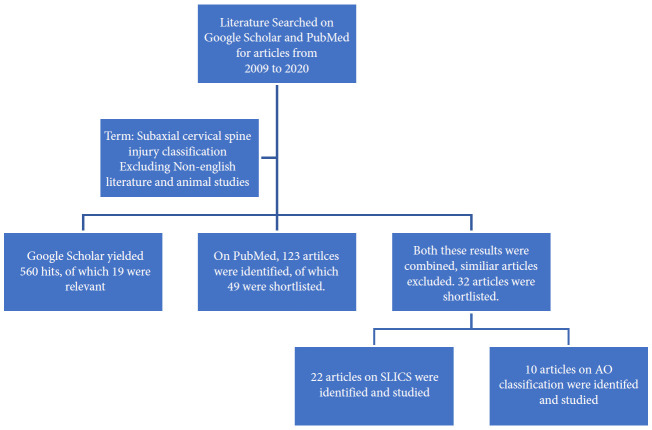
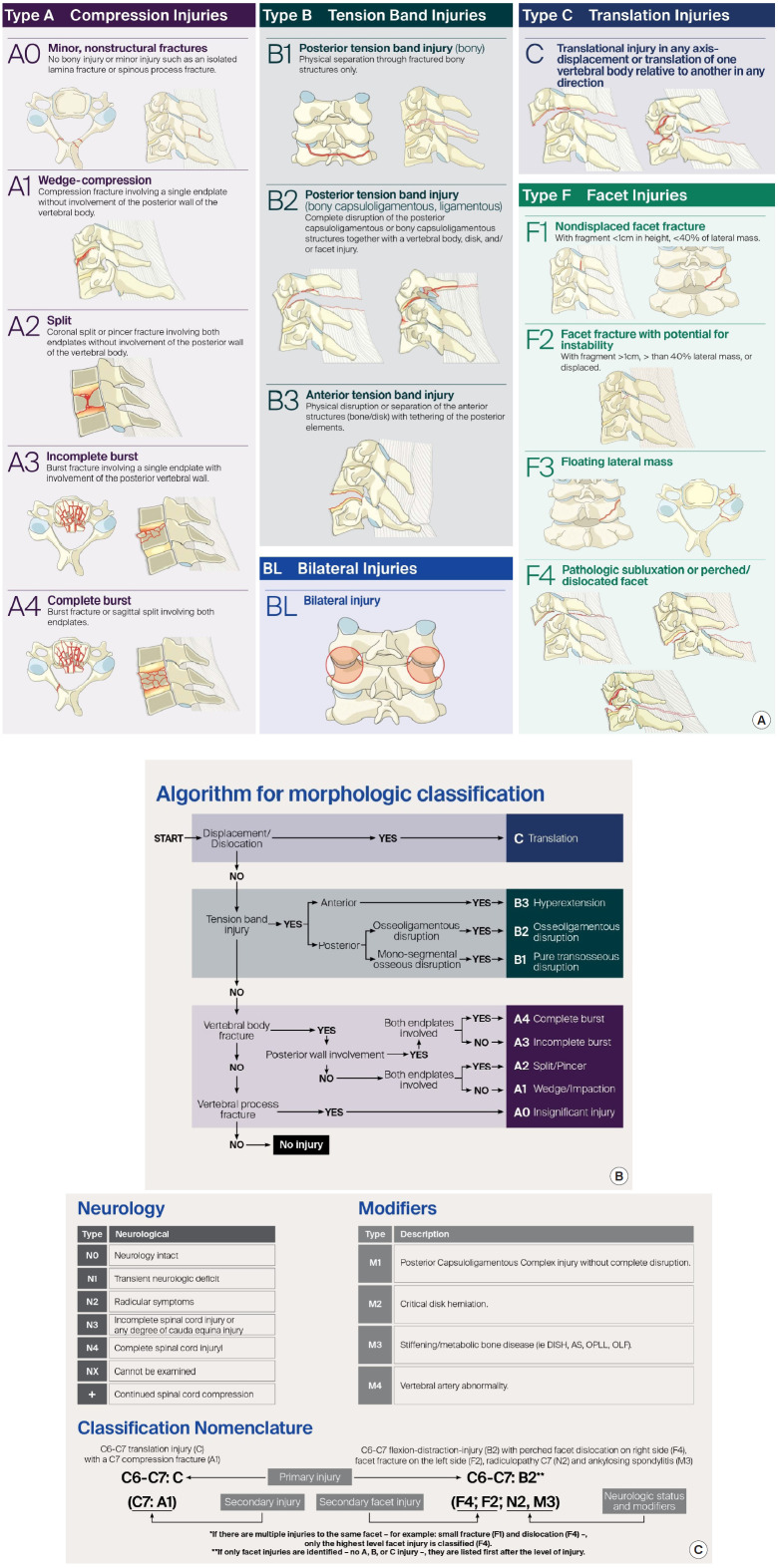
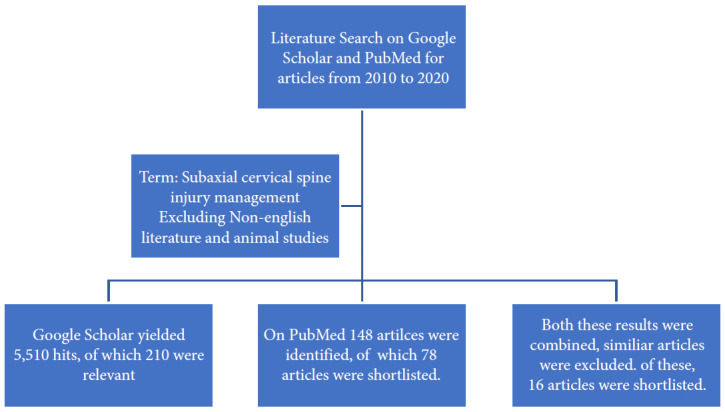
To formulate specific guidelines for the recommendation of subaxial cervical spine injuries concerning classification, management, posttraumatic locked facets and vertebral artery injury. Computerized literature was searched on PubMed and google scholar database from 2009 to 2020. For classification, keywords "Sub Axial Cervical Spine Classification," resulting in 22 articles related to subaxial cervical spine injury classification system (SLICS) system and 11 articles related to AO (Arbeitsgemeinschaft für Osteosynthesefragen, German for "Association for the Study of Internal Fixation") Spine system. The literature search yielded 210 and 78 articles on "management of subaxial cervical spine injuries" and the role of "SLICS" and "AO Spine" respectively. Keywords "management of traumatic facet locks" were searched and closed reduction, traction, approaches and techniques were studied. "Vertebral artery injury and cervical fracture" exhibited 2,328 references from the last 15 years. The objective was to identify the appropriate diagnostic tests and optimal treatment. Up-to-date information was reviewed, and statements were produced to reach a consensus in 2 separate consensus meetings of World Federation of Neurosurgical Societies (WFNS) Spine Committee. The statements were voted and reached a positive or negative consensus using Delphi method. Based on the most relevant literature, panelists in Moscow consensus meeting conducted in May 2019 drafted the statements, and after a preliminary voting session, the consensus was identified on various statements. Another meeting was conducted at Peshawar in November 2019, where in addition to previous statements, few other statements were discussed and voted. Specific recommendations were then formulated guiding classification, management, locked facets and vertebral artery injuries. This review summarizes the WFNS Spine Committee recommendations on subaxial cervical spine injuries.
Keywords: AO Spine; Classification and management; Locked facet; Subaxial cervical spine; Subaxial cervical spine injury classification system; Vertebral artery injury.
Conflict of interest statement
The authors have nothing to disclose.
Figures



Similar articles
-
Vertebral augmentation in osteoporotic spine fractures: WFNS Spine Committee recommendations.J Neurosurg Sci. 2022 Aug;66(4):311-326. doi: 10.23736/S0390-5616.22.05642-9. J Neurosurg Sci. 2022. PMID: 36153881
-
Early Management of Cervical Spine Trauma: WFNS Spine Committee Recommendations.Neurospine. 2020 Dec;17(4):710-722. doi: 10.14245/ns.2040282.141. Epub 2020 Dec 31. Neurospine. 2020. PMID: 33401852 Free PMC article.
-
Osteoporotic vertebral fractures: radiologic diagnosis, clinical and radiologic factors affecting surgical decision making: WFNS spine committee recommendations.J Neurosurg Sci. 2022 Aug;66(4):291-299. doi: 10.23736/S0390-5616.22.05636-3. Epub 2022 Mar 17. J Neurosurg Sci. 2022. PMID: 35301843 Review.
-
Establishing the Injury Severity of Subaxial Cervical Spine Trauma: Validating the Hierarchical Nature of the AO Spine Subaxial Cervical Spine Injury Classification System.Spine (Phila Pa 1976). 2021 May 15;46(10):649-657. doi: 10.1097/BRS.0000000000003873. Spine (Phila Pa 1976). 2021. PMID: 33337687 Free PMC article.
-
Developing consensus for the management of pediatric cervical spine disorders and stabilization: a modified Delphi study.J Neurosurg Pediatr. 2022 Oct 28;31(1):32-42. doi: 10.3171/2022.9.PEDS22319. Print 2023 Jan 1. J Neurosurg Pediatr. 2022. PMID: 36308472 Review.
Cited by
-
Clinical and radiological outcomes of one-level cervical corpectomy with an expandable cage for three-column uncomplicated subaxial type «B» injures: a multicenter retrospective study.Eur Spine J. 2023 May;32(5):1644-1654. doi: 10.1007/s00586-023-07648-x. Epub 2023 Mar 28. Eur Spine J. 2023. PMID: 36976341
-
Secondary Dislocations in Type B and C Injuries of the Subaxial Cervical Spine: Risk Factors and Treatment.J Clin Med. 2024 Jan 25;13(3):700. doi: 10.3390/jcm13030700. J Clin Med. 2024. PMID: 38337392 Free PMC article.
-
Concept for direct reduction of large-sized cervical tear-drop fractures through a single anterior approach with follow up of five cases.Arch Orthop Trauma Surg. 2025 Apr 19;145(1):256. doi: 10.1007/s00402-025-05875-z. Arch Orthop Trauma Surg. 2025. PMID: 40252150
-
Surgical Versus Conservative Management for Treating Unstable Atlas Fractures: A Multicenter Study.Neurospine. 2022 Dec;19(4):1013-1025. doi: 10.14245/ns.2244352.176. Epub 2022 Oct 23. Neurospine. 2022. PMID: 36274194 Free PMC article.
-
Predictors of failure after primary anterior cervical discectomy and fusion for subaxial traumatic spine injuries.Eur Spine J. 2024 Jun;33(6):2332-2339. doi: 10.1007/s00586-024-08264-z. Epub 2024 Apr 25. Eur Spine J. 2024. PMID: 38664273
References
-
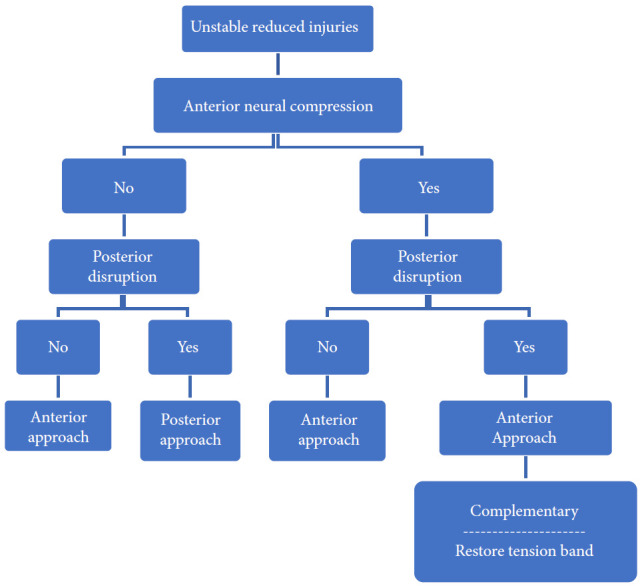
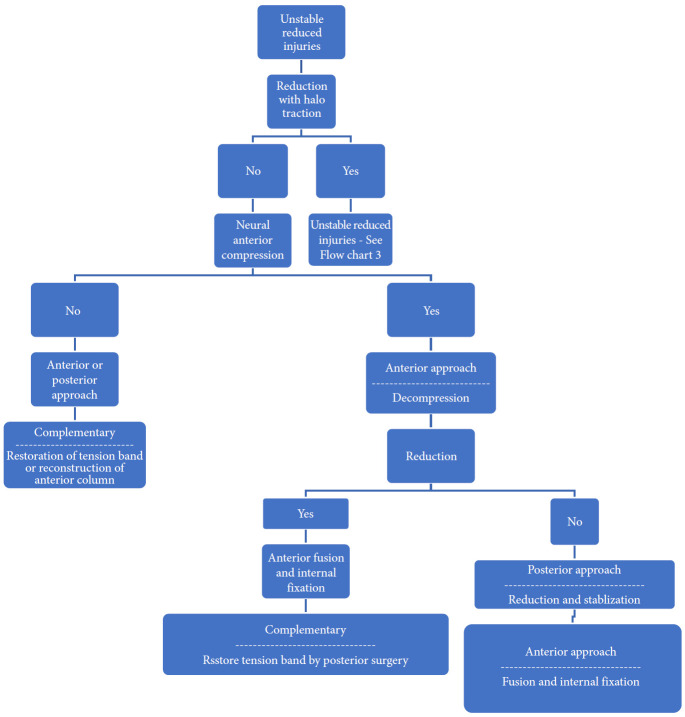
- Dvorak MF, Fisher CG, Fehlings MG, et al. The surgical approach to subaxial cervical spine injuries: an evidence-based algorithm based on the SLIC classification system. Spine (Phila Pa 1976) 2007;32:2620–9. - PubMed
-
- Lebl DR, Bono CM, Velmahos G, et al. Vertebral artery injury associated with blunt cervical spine trauma: a multivariate regression analysis. Spine (Phila Pa 1976) 2013;38:1352–61. - PubMed
-
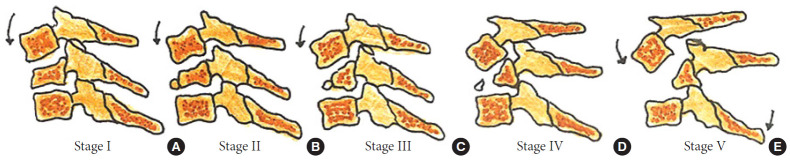
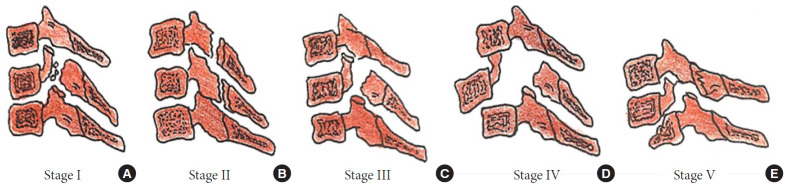
- Allen BL, Jr, Ferguson RL, Lehmann TR, et al. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine (Phila Pa 1976) 1982;7:1–27. - PubMed
LinkOut - more resources
Full Text Sources
