

Chronic Opioid Use Following Lumbar Discectomy: Prevalence, Risk Factors, and Current Trends in the United States
- PMID: 33401866
- PMCID: PMC7788426
- DOI: 10.14245/ns.2040122.061
Chronic Opioid Use Following Lumbar Discectomy: Prevalence, Risk Factors, and Current Trends in the United States
Abstract
Objective: Lumbar discectomy is commonly performed for symptomatic lumbar disc herniation. We aimed to examine prescribing patterns and risk factors for chronic opioid use following lumbar discectomy.
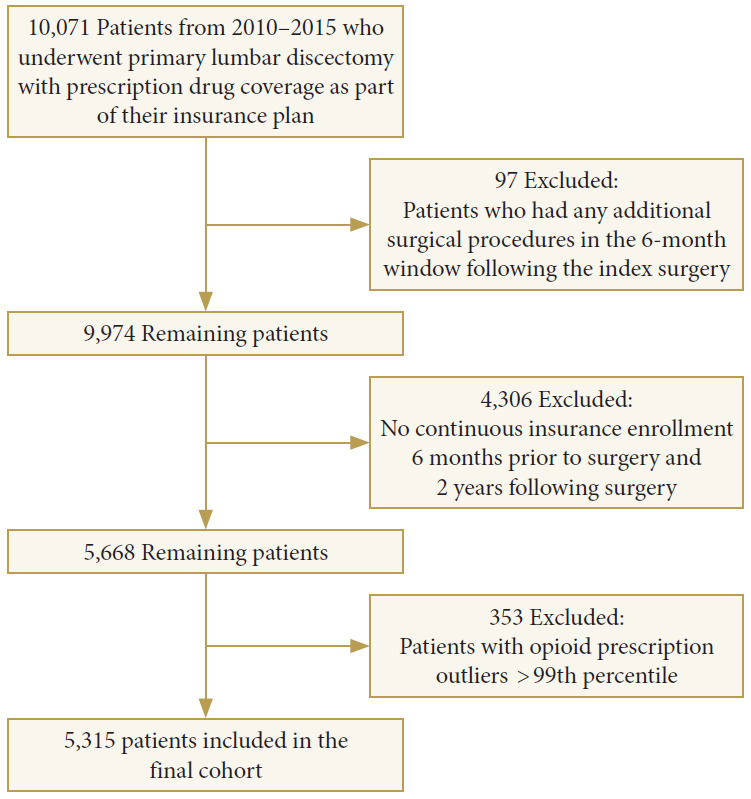
Methods: Using a private insurance claims database, patients were identified who underwent primary lumbar discectomy from 2010-2015 and had 1-year of continuous enrollment postoperatively. Patients were excluded with spinal fusion. The strength of opioid prescriptions was quantified using morphine milligram equivalents daily (MMED). Univariate and multivariate logistic regression models were built to examine risk factors associated with chronic postoperative opioid use.
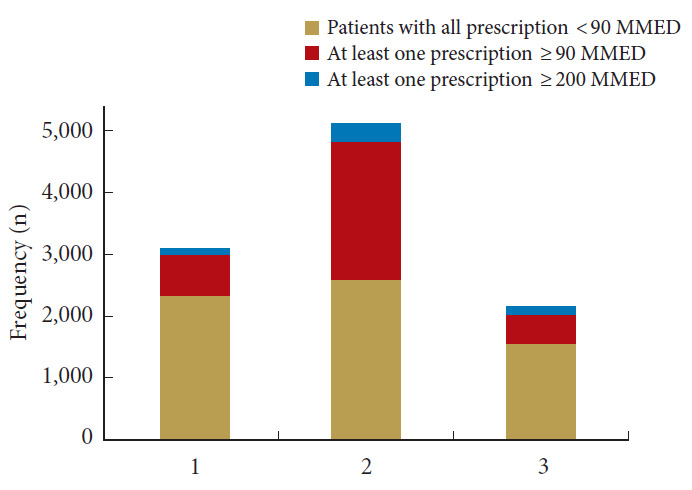
Results: A total of 5,315 patients were included in the study (mean age, 59 years; 50% female). 1,198 of patients (23%) used chronic opioids postoperatively. Chronic opioid use declined significantly from 27% in 2010 to 17% in 2015, p < 0.001. In addition, there were significantly fewer patients receiving high and very high-dose opioid prescriptions from 2010-2015, p < 0.001. The median duration that patients used opioids postoperatively was 211 days in 2010 (interquartile range [IQR], 29-356 days), and decreased significantly to 44 days (IQR, 10-294 days) in 2015. The strongest factors associated with chronic opioid use were preoperative opioid use (odds ratio [OR], 4.0), drug abuse (OR, 2.6), depression (OR, 1.6), surgery in the west (OR, 1.6) or south (OR, 1.6), anxiety (OR, 1.5), or 30-day readmission (OR, 1.4).
Conclusion: Chronic opioid use following primary lumbar discectomy has declined from 2010-2015. A variety of factors are associated with chronic opioid use. Preoperative recognition of some of these risk factors may aid in perioperative management and counseling.
Keywords: Diskectomy; Lumbar vertebrae; Opioid analgesics; Prevalence; Risk factor.
Conflict of interest statement
Dr. Bicket reports Axial Healthcare (past service on advisory board, stock options) and Alosa (advisory board). Except for that, the authors have nothing to disclose.
Figures
Similar articles
-
Chronic opioid use following anterior cervical discectomy and fusion surgery for degenerative cervical pathology.Spine J. 2020 Jan;20(1):78-86. doi: 10.1016/j.spinee.2019.09.011. Epub 2019 Sep 16. Spine J. 2020. PMID: 31536805
-
Burden of preoperative opioid use and its impact on healthcare utilization after primary single level lumbar discectomy.Spine J. 2021 Oct;21(10):1700-1710. doi: 10.1016/j.spinee.2021.04.013. Epub 2021 Apr 17. Spine J. 2021. PMID: 33872806
-
Effect of narcotic prescription limiting legislation on opioid utilization following lumbar spine surgery.Spine J. 2019 Apr;19(4):717-725. doi: 10.1016/j.spinee.2018.09.007. Epub 2018 Sep 14. Spine J. 2019. PMID: 30223089
-
Opioid prescribing practices after posterior spinal arthrodesis for adolescent idiopathic scoliosis.Spine Deform. 2020 Oct;8(5):965-973. doi: 10.1007/s43390-020-00127-z. Epub 2020 May 6. Spine Deform. 2020. PMID: 32378042
-
Incidence and risk factors for prolonged postoperative opioid use following lumbar spine surgery: a cohort study.J Neurosurg Spine. 2021 Aug 6;35(5):583-591. doi: 10.3171/2021.2.SPINE202205. Print 2021 Nov 1. J Neurosurg Spine. 2021. PMID: 34359026
Cited by
-
Biportal Endoscopic Spine Surgery for Lumbar Laminectomy and Diskectomy: Postoperative Outcomes and Surgical Learning Curve, a Single US Surgeon's Experience.J Am Acad Orthop Surg Glob Res Rev. 2024 Aug 19;8(8):e23.00161. doi: 10.5435/JAAOSGlobal-D-23-00161. eCollection 2024 Aug 1. J Am Acad Orthop Surg Glob Res Rev. 2024. PMID: 39162736 Free PMC article.
-
Association Between Early Surgery and Postoperative Opioid Use in Patients With Lumbar Disc Herniation: A Propensity Score-Matching Analysis Using an Administrative Claims Database in Japan.Global Spine J. 2024 Jul;14(6):1738-1744. doi: 10.1177/21925682231154854. Epub 2023 Jan 25. Global Spine J. 2024. PMID: 36696513 Free PMC article.
-
Trends of opioid use following anterior cervical discectomy and fusion: A 10-year longitudinal study of the Veterans Health Administration.N Am Spine Soc J. 2025 Feb 8;22:100595. doi: 10.1016/j.xnsj.2025.100595. eCollection 2025 Jun. N Am Spine Soc J. 2025. PMID: 40160480 Free PMC article.
-
A study on the 10-year trend of surgeries performed for lumbar disc herniation and comparative analysis of prescribed opioid analgesics and hospitalization duration: 2010-2019 HIRA NPS Data.BMC Musculoskelet Disord. 2024 Jan 13;25(1):65. doi: 10.1186/s12891-024-07167-w. BMC Musculoskelet Disord. 2024. PMID: 38218767 Free PMC article.
-
Opioid-use disorder and reported pain after spine surgery: Risk-group patterns in cognitive-appraisal processes in a longitudinal cohort study.N Am Spine Soc J. 2025 Mar 12;22:100605. doi: 10.1016/j.xnsj.2025.100605. eCollection 2025 Jun. N Am Spine Soc J. 2025. PMID: 40256050 Free PMC article.
References
-
- O’Donnell JA, Anderson JT, Haas AR, et al. Preoperative opioid use is a predictor of poor return to work in workers’ compensation patients after lumbar diskectomy. Spine (Phila Pa 1976) 2018;43:594–602. - PubMed
-
- Williams RW. Microlumbar discectomy. A 12-year statistical review. Spine (Phila Pa 1976) 1986;11:851–2. - PubMed
-
- Moore AJ, Chilton JD, Uttley D. Long-term results of microlumbar discectomy. Br J Neurosurg. 1994;8:319–26. - PubMed
-
- Harrington JF, French P. Open versus minimally invasive lumbar microdiscectomy: comparison of operative times, length of hospital stay, narcotic use and complications. Minim Invasive Neurosurg. 2008;51:30–5. - PubMed
LinkOut - more resources
Full Text Sources
