

Evaluation of the optical criteria for sessile serrated lesions of the colon: A prospective study on a colorectal cancer screening population
- PMID: 33403231
- PMCID: PMC7775808
- DOI: 10.1055/a-1293-7086
Evaluation of the optical criteria for sessile serrated lesions of the colon: A prospective study on a colorectal cancer screening population
Abstract
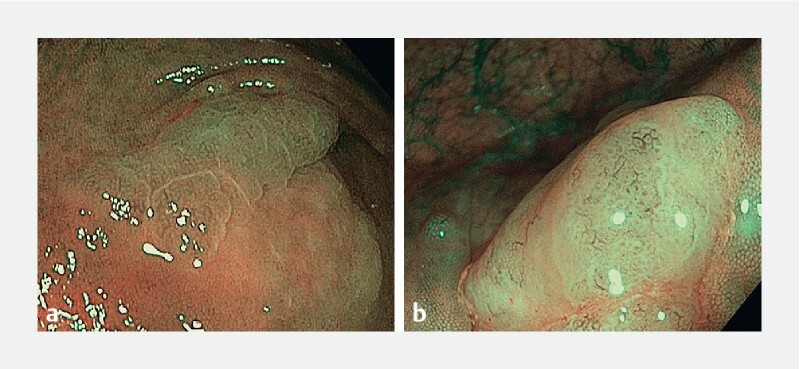
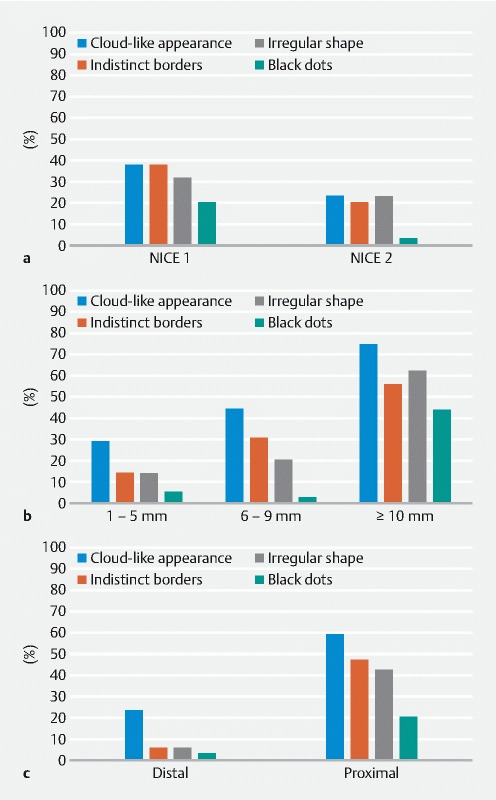
Background and study aims We aimed to describe the presence and combination of Hazewinkel's optical diagnosis (OD) criteria for sessile serrated lesions (SSL), determining which lesion characteristics increase the probability of a correct OD, with a focus on diminutive lesions. Patients and methods This was a prospective study describing the presence of Hazewinkel's OD criteria for SSL in lesions found in consecutive CRC screening colonoscopies. The presence of each OD criterion and their diagnostic combinations in SSL, related to the lesion's NBI International Colorectal Endoscopic (NICE) classification category, size, and location, were described. The presence of two or more optical criteria was considered diagnostic of SSL. The OD was compared to pathology as the gold standard. Results Seventy-nine SSLs (5.6 %) were diagnosed. Cloud-like appearance was the most prevalent OD criterion (35, 44.3 %). OD criteria were more frequently identified in NICE type 1, ≥ 10 mm, and proximal lesions. Only 26 SLLs fulfilled the OD criteria (sensitivity 32.9 %, 95 % CI 29.1 %-36.7 %). The sensitivity for diminutive SSL was 14.7 %, (95 % CI 11.9 %-17.6 %). Eighty-five lesions were optically diagnosed as SSL. However, only in 26 SSL was this the definitive diagnosis (positive predictive value 30.6 %, 95 % CI 26.9 %-34.3 %). Size > 5 mm and proximal location increased the probability of a correct diagnosis. The overall accuracy of the optical criteria was 92.0 % (95 % CI, 89.8 %-94.2 %). Conclusions The Hazewinkel's optical criteria are not reliable for a positive diagnosis of SSL, particularly for diminutive lesions.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests The authors declare that they have no conflict of interest.
Figures
References
-
- Snover D C. Update on the serrated pathway to colorectal carcinoma. Hum Pathol. 2011;42:1–10. - PubMed
-
- Pohl H, Srivastava A, Bensen S P et al. Incomplete polyp resection during colonoscopy-results of the complete adenoma resection (CARE) study. Gastroenterology. 2013;144:74–80 e71. - PubMed
-
- Oono Y, Fu K, Nakamura H et al. Progression of a sessile serrated adenoma to an early invasive cancer within 8 months. Digest Dis Sci. 2009;54:906–909. - PubMed
-
- Rex D K, Kahi C, OʼBrien M et al. The American Society for Gastrointestinal Endoscopy PIVI (Preservation and Incorporation of Valuable Endoscopic Innovations) on real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest Endosc. 2011;73:419–422. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources