

Allogeneic Mesenchymal Cell Therapy in Anthracycline-Induced Cardiomyopathy Heart Failure Patients: The CCTRN SENECA Trial
- PMID: 33403362
- PMCID: PMC7781291
- DOI: 10.1016/j.jaccao.2020.09.001
Allogeneic Mesenchymal Cell Therapy in Anthracycline-Induced Cardiomyopathy Heart Failure Patients: The CCTRN SENECA Trial
Abstract
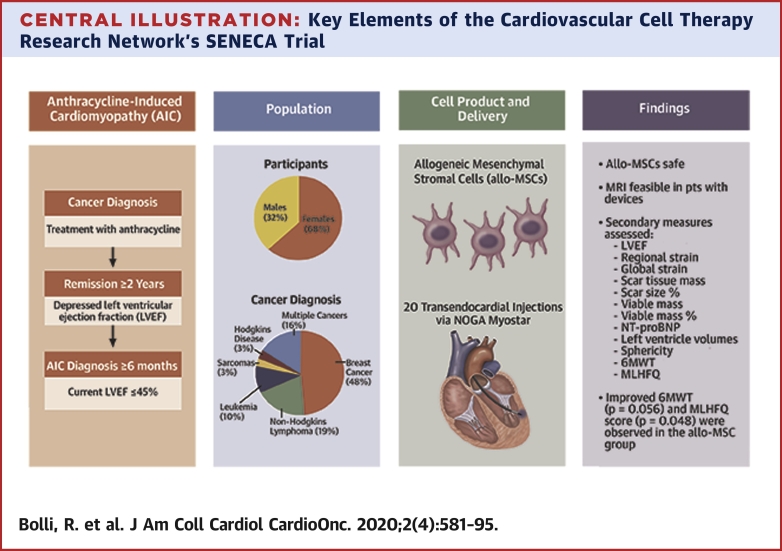
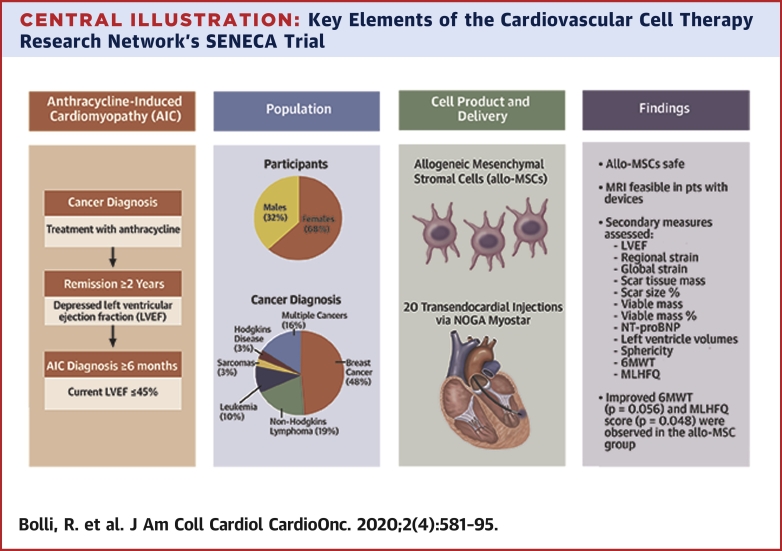
Background: Anthracycline-induced cardiomyopathy (AIC) may be irreversible with a poor prognosis, disproportionately affecting women and young adults. Administration of allogeneic bone marrow-derived mesenchymal stromal cells (allo-MSCs) is a promising approach to heart failure (HF) treatment.
Objectives: SENECA (Stem Cell Injection in Cancer Survivors) was a phase 1 study of allo-MSCs in AIC.
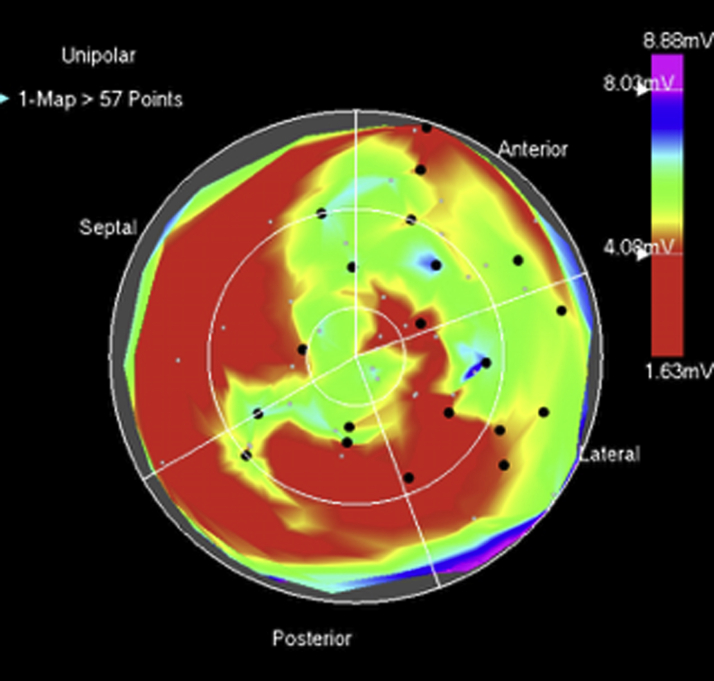
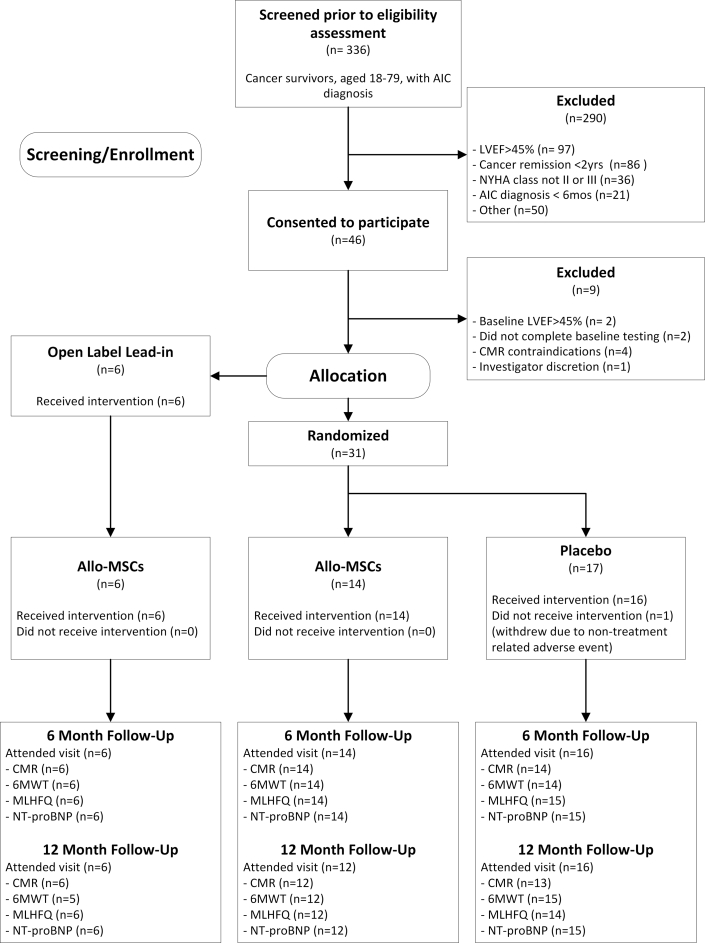
Methods: Cancer survivors with chronic AIC (mean age 56.6 years; 68% women; NT-proBNP 1,426 pg/ml; 6 enrolled in an open-label, lead-in phase and 31 subjects randomized 1:1) received 1 × 108 allo-MSCs or vehicle transendocardially. Primary objectives were safety and feasibility. Secondary efficacy measures included cardiac function and structure measured by cardiac magnetic resonance imaging (CMR), functional capacity, quality of life (Minnesota Living with Heart Failure Questionnaire), and biomarkers.
Results: A total of 97% of subjects underwent successful study product injections; all allo-MSC-assigned subjects received the target dose of cells. Follow-up visits were well-attended (92%) with successful collection of endpoints in 94% at the 1-year visit. Although 58% of subjects had non-CMR compatible devices, CMR endpoints were successfully collected in 84% of subjects imaged at 1 year. No new tumors were reported. There were no significant differences between allo-MSC and vehicle groups with regard to clinical outcomes. Secondary measures included 6-min walk test (p = 0.056) and Minnesota Living with Heart Failure Questionnaire score (p = 0.048), which tended to favor the allo-MSC group.
Conclusions: In this first-in-human study of cell therapy in patients with AIC, transendocardial administration of allo-MSCs appears safe and feasible, and CMR was successfully performed in the majority of the HF patients with devices. This study lays the groundwork for phase 2 trials aimed at assessing efficacy of cell therapy in patients with AIC.
Keywords: cardiac repair; cardiooncology; chemotherapy; heart failure; stem cells.
Conflict of interest statement
This work is supported by the National Institutes of Health (5 UM1 HL087318). All investigators received funding from the NIH National Heart, Lung, and Blood Institute (NHLBI) for conduct of the SENECA trial through the Cardiovascular Cell Therapy Research Network (CCTRN). Dr. Hare has held stock in Longeveron; has held stock and intellectual property in Vestion; and has a grant with Biologics Delivery Systems. Dr. Henry has served as a consultant for Biosense Webster. Dr. Pepine has served as a consultant for XyloCor, Caladrius, Imbria, and Biocardia; and has grants with Adelphi Values, Brigham and Women’s Hospital, Department of Defense, Gilead Sciences, Inc., McJunkin Foundation, Mesoblast, and Sanofi US. Dr. Perin has served as a consultant for Mesoblast. Dr. Taylor is co-founder of Stem Cell Security. Dr. Yang has served as a consultant for Terumo. Dr. Ebert has served as a staff member of the National Heart, Lung, and Blood Institute, the source of funding for the SENECA trial. The views expressed in this article are those of the authors and do not necessarily represent the views of the NHLBI, National Institutes of Health, or the United States Department of Health and Human Services. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
One Small Step . .JACC CardioOncol. 2020 Nov 17;2(4):596-598. doi: 10.1016/j.jaccao.2020.10.003. eCollection 2020 Nov. JACC CardioOncol. 2020. PMID: 34396270 Free PMC article.
References
-
- Steinherz L.J., Steinherz P.G., Tan C.T., Heller G., Murphy M.L. Cardiac toxicity 4 to 20 years after completing anthracycline therapy. JAMA. 1991;266:1672–1677. - PubMed
-
- Cardinale D., Colombo A., Lamantia G. Anthracycline-induced cardiomyopathy: clinical relevance and response to pharmacologic therapy. J Am Coll Cardiol. 2010;55:213–220. - PubMed
-
- Shan K., Lincoff A.M., Young J.B. Anthracycline-induced cardiotoxicity. Ann Intern Med. 1996;125:47–58. - PubMed
-
- Billingham M.E., Mason J.W., Bristow M.R., Daniels J.R. Anthracycline cardiomyopathy monitored by morphologic changes. Cancer Treat Rep. 1978;62:865–872. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
