

Initial findings in traumatic peripheral nerve injury and repair with diffusion tensor imaging
- PMID: 33403827
- PMCID: PMC7886047
- DOI: 10.1002/acn3.51270
Initial findings in traumatic peripheral nerve injury and repair with diffusion tensor imaging
Abstract
Objective: Management of peripheral nerve injuries requires physicians to rely on qualitative measures from patient history, electromyography, and physical exam. Determining a successful nerve repair can take months to years for proximal injuries, and the resulting delays in clinical decision-making can lead to a negative impact on patient outcomes. Early identification of a failed nerve repair could prevent permanent muscle atrophy and loss of function. This study aims to test the feasibility of performing diffusion tensor imaging (DTI) to evaluate injury and recovery following repair of wrist trauma. We hypothesize that DTI provides a noninvasive and reliable assessment of regeneration, which may improve clinical decision-making and alter the clinical course of surgical interventions.
Methods: Clinical and MRI measurements from subjects with traumatic peripheral nerve injury, carpal tunnel syndrome, and healthy control subjects were compared to evaluate the relationship between DTI metrics and injury severity.
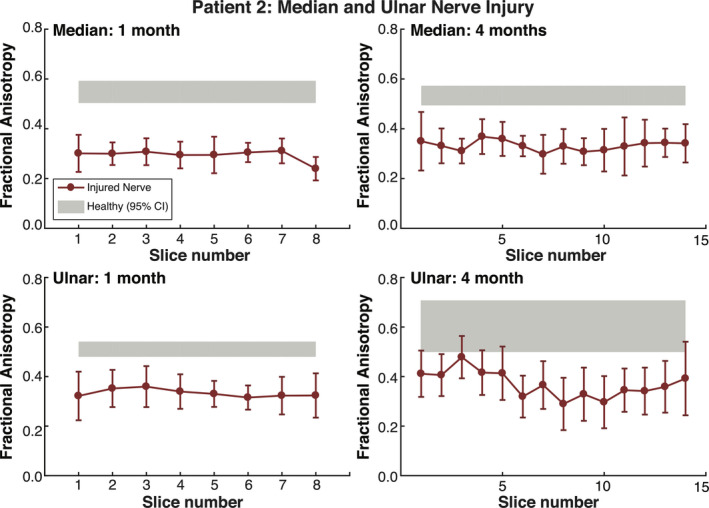
Results: Fractional anisotropy from DTI was sensitive to differences between damaged and healthy nerves, damaged and compressed nerves, and injured and healthy contralateral nerves. Longitudinal measurements in two injury subjects also related to clinical outcomes. Implications of other diffusion measures are also discussed.
Interpretation: DTI is a sensitive tool for wrist nerve injuries and can be utilized for monitoring nerve recovery. Across three subjects with nerve injuries, this study has shown how DTI can detect abnormalities between injured and healthy nerves, measure recovery, and determine if re-operation was successful. Additional comparisons to carpal tunnel syndrome and healthy nerves show that DTI is sensitive to the degree of impairment.
© 2021 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
No authors in this manuscript have any conflict of interest to disclose.
Figures







References
-
- Noble J, Munro CA, Prasad VSSV, Midha R. Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. J Trauma ‐ Inj Infect Crit Care 1998;45:116–122. - PubMed
-
- Cross JD, Ficke JR, Hsu JR, et al. Battlefield orthopaedic injuries cause the majority of long‐term disabilities. J Am Acad Orthop Surg 2011;19:1–7. - PubMed
-
- Stansbury LG, Branstetter JG, Lalliss SJ. Amputation in military trauma surgery. J Trauma ‐ Inj Infect Crit Care 2007;63:940–944. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical