

Hospital volume is associated with postoperative mortality after radical cystectomy for treatment of bladder cancer
- PMID: 33404154
- PMCID: PMC8519083
- DOI: 10.1111/bju.15334
Hospital volume is associated with postoperative mortality after radical cystectomy for treatment of bladder cancer
Abstract
Objective: To contribute to the debate regarding the minimum volume of radical cystectomies (RCs) that a hospital should perform by evaluating the association between hospital volume (HV) and postoperative mortality.
Patients and methods: Patients who underwent RC for bladder cancer between 1 January 2008 and 31 December 2018 were retrospectively identified from the Netherlands Cancer Registry. To create a calendar-year independent measure, the HV of RCs was calculated per patient by counting the RCs performed in the same hospital in the 12 months preceding surgery. The relationship of HV with 30- and 90-day mortality was assessed by logistic regression with a non-linear spline function for HV as a continuous variable, which was adjusted for age, tumour, node and metastasis (TNM) stage, and neoadjuvant treatment.
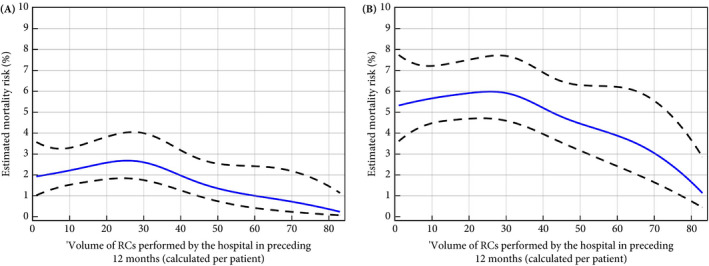
Results: The median (interquartile range; range) HV among the 9287 RC-treated patients was 19 (12-27; 1-75). Of all the included patients, 208 (2.2%) and 518 (5.6%) died within 30 and 90 days after RC, respectively. After adjustment for age, TNM stage and neoadjuvant therapy, postoperative mortality slightly increased between an HV of 0 and an HV of 25 RCs and steadily decreased from an HV of 30 onwards. The lowest risks of postoperative mortality were observed for the highest volumes.
Conclusion: This paper, based on high-quality data from a large nationwide population-based cohort, suggests that increasing the RC volume criteria beyond 30 RCs annually could further decrease postoperative mortality. Based on these results, the volume criterion of 20 RCs annually, as recently recommended by the European Association of Urology Guideline Panel, might therefore be reconsidered.
Keywords: #BladderCancer; #blcsm; #uroonc; bladder cancer; hospital volume; postoperative mortality; radical cystectomy.
© 2021 The Authors BJU International published by John Wiley & Sons Ltd on behalf of BJU International.
Conflict of interest statement
None declared.
Figures


References
-
- Witjes JA, Lebret T, Compérat EM et al. Updated 2016 EAU guidelines on muscle‐invasive and metastatic bladder cancer. Eur Urol 2017; 71: 462–75 - PubMed
-
- Goossens‐Laan CA, Gooiker GA, van Gijn W et al. A systematic review and meta‐analysis of the relationship between hospital/surgeon volume and outcome for radical cystectomy: an update for the ongoing debate. Eur Urol 2011; 59: 775–83 - PubMed
-
- Nederlandse Vereniging van Urologie, Kwaliteitsnorm blaascarcinoom, 2018.
-
- Afshar M, Goodfellow H, Jackson‐Spence F et al. Centralisation of radical cystectomies for bladder cancer in England, a decade on from the 'Improving Outcomes Guidance': the case for super centralisation. BJU Int 2018; 121: 217–24 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
