

Evaluation of Dietary Niacin and New-Onset Hypertension Among Chinese Adults
- PMID: 33404619
- PMCID: PMC7788463
- DOI: 10.1001/jamanetworkopen.2020.31669
Evaluation of Dietary Niacin and New-Onset Hypertension Among Chinese Adults
Abstract
Importance: The relationship of dietary niacin intake with the risk of hypertension remains unknown.
Objective: To determine the prospective association between dietary niacin intake and new-onset hypertension, and examine factors that may modify the association among Chinese adults.
Design, setting, and participants: This nationwide cohort study of 12 243 Chinese adults used dietary intake data from 7 rounds of the China Health and Nutrition Survey. Dietary intake was measured by 3 consecutive 24-hour dietary recalls from participants in combination with a weighing inventory taken over the same 3 days at the household level. Statistical analysis was conducted from May 2020 to August 2020.
Exposures: Dietary intake.
Main outcomes and measures: The study outcome was new-onset hypertension, defined as systolic blood pressure 140 mm Hg or greater and/or diastolic blood pressure 90 mm Hg or greater, diagnosis by physician, or current antihypertensive treatment during the follow-up.
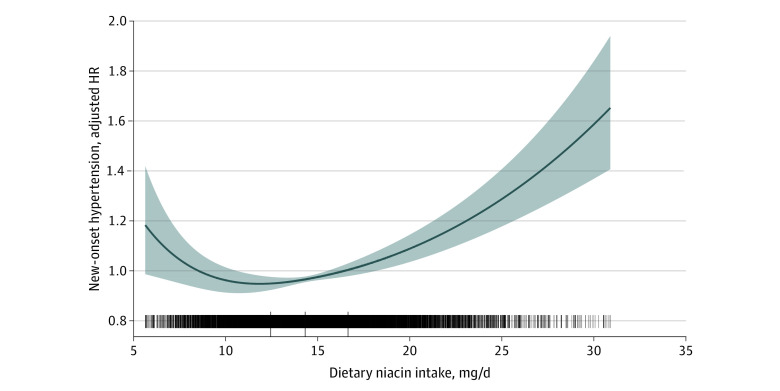
Results: The mean (SD) age of the study population was 41.2 (14.2) years, and 5728 (46.8%) of participants were men. The mean (SD) dietary niacin intake level was 14.8 (4.1) mg/d. A total of 4306 participants developed new-onset hypertension during a median (interquartile range) follow-up duration of 6.1 (3.6-11.3) years. When dietary niacin was assessed in quartiles, the lowest risk of new-onset hypertension was found in participants in quartile 3 (14.3 to <16.7 mg/d; adjusted hazard ratio, 0.83; 95% CI, 0.75-0.90) compared with those in quartile 1 (<12.4 mg/d). Consistently in the threshold analysis, for every 1 mg/d increase in dietary niacin, there was a 2% decrease in new-onset hypertension (adjusted HR, 0.98; 95% CI, 0.96-1.00) in those with dietary niacin intake less than 15.6 mg/d, and a 3% increase in new-onset hypertension (adjusted HR, 1.03; 95% CI, 1.02-1.04) in participants with dietary niacin 15.6 mg/d or greater. Based on these results, there was a J-shaped association between dietary niacin intake and new-onset hypertension in the general population of Chinese adults, with an inflection point at 15.6 mg/d and a minimal risk at 14.3 to 16.7 mg/d (quartile 3) of dietary niacin intake.
Conclusions and relevance: The results of this study provide some evidence for maintaining the optimal dietary niacin intake levels for the primary prevention of hypertension.
Conflict of interest statement
Figures
References
-
- GBD 2017 Risk Factor Collaborators Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1923-1994. doi: 10.1016/S0140-6736(18)32225-6 - DOI - PMC - PubMed
-
- Li Y, Zhou H, Liu M, et al. Association of visit-to-visit variability in blood pressure and first stroke risk in hypertensive patients with chronic kidney disease. J Hypertens. 2020;38(4):610-617. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
