

Patient Factors Associated With Parathyroidectomy in Older Adults With Primary Hyperparathyroidism
- PMID: 33404646
- PMCID: PMC7788507
- DOI: 10.1001/jamasurg.2020.6175
Patient Factors Associated With Parathyroidectomy in Older Adults With Primary Hyperparathyroidism
Abstract
Importance: Parathyroidectomy provides definitive management for primary hyperparathyroidism (PHPT), reducing the risk of subsequent fracture, nephrolithiasis, and chronic kidney disease (CKD), but its use among older adults in the US is unknown.
Objective: To identify patient characteristics associated with the use of parathyroidectomy for the management of PHPT in older adults.
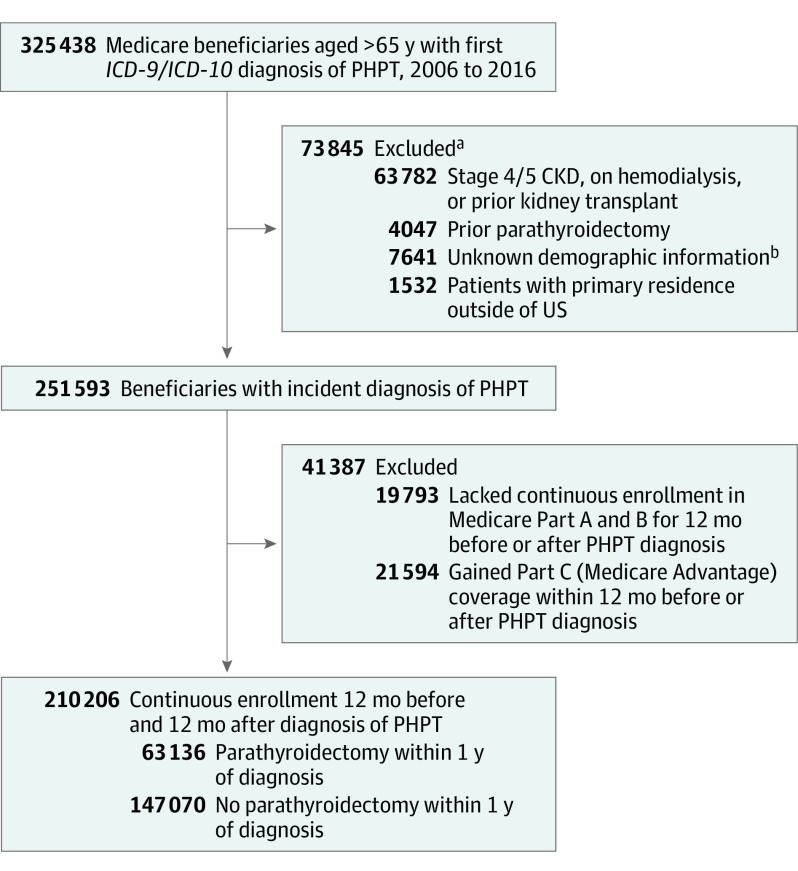
Design, setting, and participants: This population-based, retrospective cohort study used 100% Medicare claims from beneficiaries with an initial diagnosis of PHPT from January 1, 2006, to December 31, 2016. Patients were considered to meet consensus guideline criteria for parathyroidectomy based on diagnosis codes indicating osteoporosis, nephrolithiasis, or stage 3 CKD. Multivariable logistic regression was used to identify patient characteristics associated with parathyroidectomy. Data were analyzed from February 11, 2020, to October 8, 2020.
Main outcomes and measures: The primary outcome was parathyroidectomy within 1 year of diagnosis.
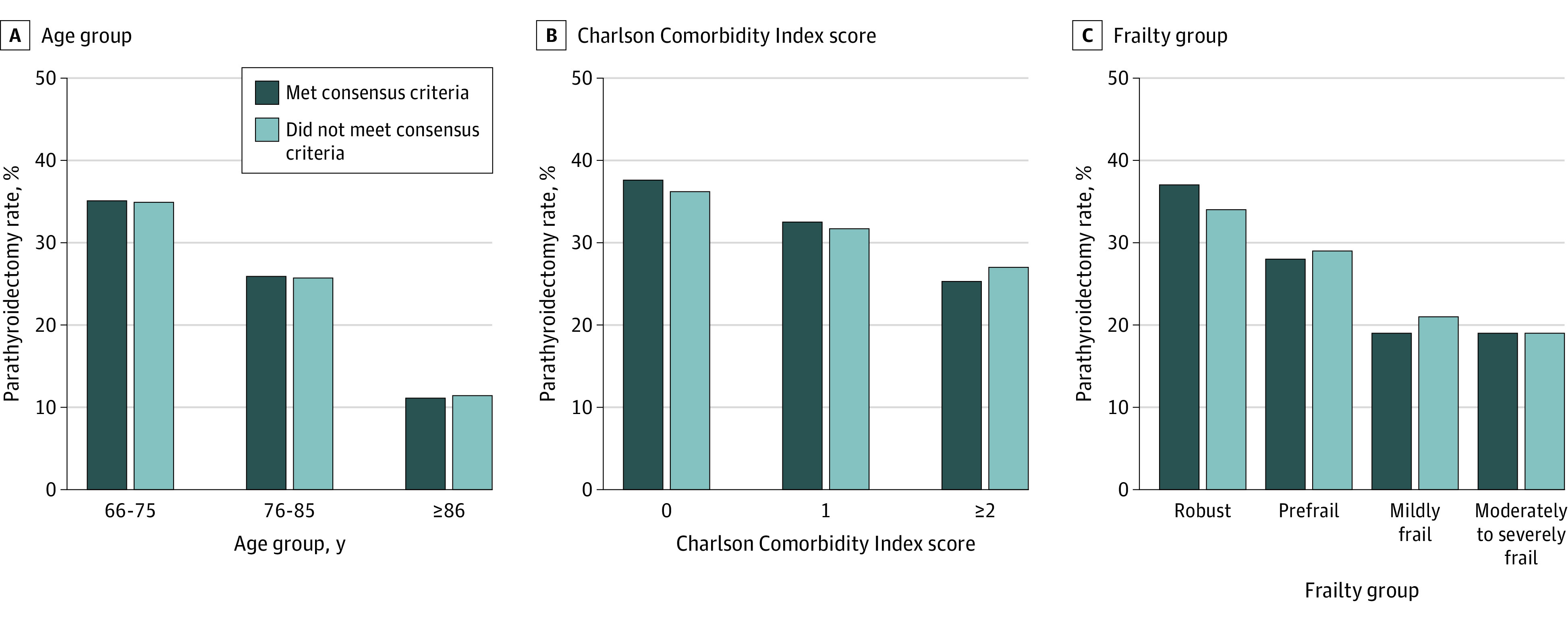
Results: Among 210 206 beneficiaries with an incident diagnosis of PHPT (78.8% women; mean [SD] age, 75.3 [6.8] years), 63 136 (30.0%) underwent parathyroidectomy within 1 year of diagnosis. Among the subset of patients who met consensus guideline criteria for operative management (n = 131 723), 38 983 (29.6%) were treated with parathyroidectomy. Patients treated operatively were younger (mean [SD] age, 73.5 [5.7] vs 76.0 [7.1] years) and more likely to be White (90.1% vs 86.0%), to be robust or prefrail (92.1% vs 85.7%), and to have fewer comorbidities (Charlson Comorbidity Index score of 0 or 1, 54.6% vs 44.1%), in addition to being more likely to live in socioeconomically disadvantaged (46.9% vs 40.3%) and rural (18.1% vs 13.6%) areas (all P < .001). On multivariable analysis, increasing age had a strong inverse association with parathyroidectomy among patients aged 76 to 85 years (unadjusted rate, 25.9%; odds ratio [OR], 0.68 [95% CI, 0.67-0.70]) and older than 85 years (unadjusted rate, 11.2%; OR, 0.27 [95% CI, 0.26-0.29]) compared with those aged 66 to 75 years (unadjusted rate, 35.6%), as did patients with moderate to severe frailty (unadjusted rate, 18.9%; OR, 0.60 [95% CI, 0.56-0.64]) compared with robust patients (unadjusted rate, 36.1%) and those with a Charlson Comorbidity Index score of 2 or greater (unadjusted rate, 25.9%; OR, 0.77 [95% CI, 0.75-0.79]) compared with a Charlson Comorbidity Index score of 0 (unadjusted rate, 37.0%). With regard to operative guidelines, a history of nephrolithiasis increased the odds of parathyroidectomy (OR, 1.43 [95% CI, 1.39-1.47]); stage 3 CKD decreased the odds of parathyroidectomy (OR, 0.71 [95% CI, 0.68-0.74]); and osteoporosis showed no association (OR, 1.01 [95% CI, 0.99-1.03]).
Conclusions and relevance: In this cohort study, most older adults with PHPT did not receive definitive treatment with parathyroidectomy. Older age, frailty, and multimorbidity were associated with nonoperative management, and guideline recommendations had minimal effect on treatment decisions. Further research is needed to identify barriers to surgical care and develop tools to target parathyroidectomy to older adults most likely to benefit.
Conflict of interest statement
Figures
Comment in
-
Undertreatment of Primary Hyperparathyroidism.JAMA Surg. 2021 Apr 1;156(4):342. doi: 10.1001/jamasurg.2020.6239. JAMA Surg. 2021. PMID: 33404591 No abstract available.
-
Urolithiasis/Endourology.J Urol. 2021 Dec;206(6):1513-1515. doi: 10.1097/JU.0000000000002207. Epub 2021 Sep 8. J Urol. 2021. PMID: 34494454 No abstract available.
References
-
- Coker LH, Rorie K, Cantley L, et al. . Primary hyperparathyroidism, cognition, and health-related quality of life. Ann Surg. 2005;242(5):642-650. doi:10.1097/01.sla.0000186337.83407.ec - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
