

Impact of primary care involvement and setting on multidisciplinary heart failure management: a systematic review and meta-analysis
- PMID: 33405392
- PMCID: PMC8006678
- DOI: 10.1002/ehf2.13152
Impact of primary care involvement and setting on multidisciplinary heart failure management: a systematic review and meta-analysis
Abstract
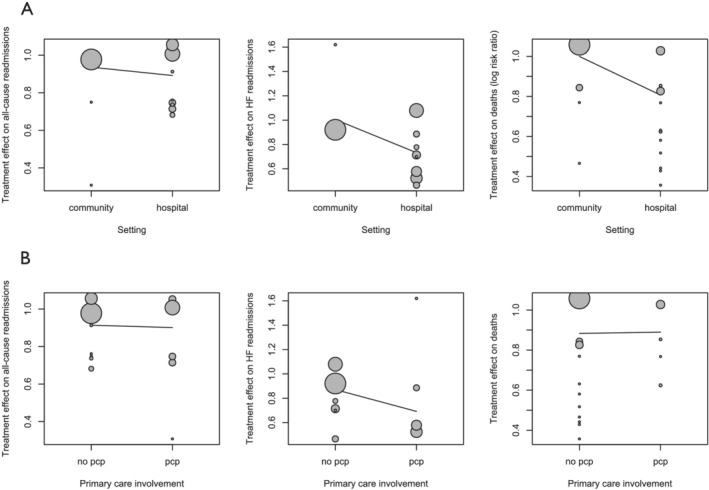
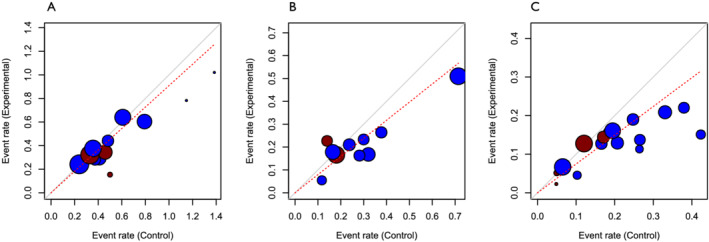
Multidisciplinary disease management programmes (DMPs) are a cornerstone of modern guideline-recommended care for heart failure (HF). Few programmes are community initiated or involve primary care professionals, despite the importance of home-based care for HF. We compared the outcomes of different multidisciplinary HF DMPs in relation to their recruitment setting and involvement of primary care health professionals. We conducted a systematic review and meta-analysis of randomized controlled trials published in MEDLINE, Embase, and Cochrane between 2000 and 2020 using Cochrane Collaboration methodology. Our meta-analysis included 19 randomized controlled trials (7577 patients), classified according to recruitment setting and involvement of primary care professionals. Thirteen studies recruited in the hospital (n = 5243 patients) and six in the community (n = 2334 patients). Only six studies involved primary care professionals (n = 3427 patients), with two of these recruited in the community (n = 225 patients). Multidisciplinary HF DMPs that recruited in the community had no significant effect on all-cause and HF readmissions nor on mortality, irrespective of primary care involvement. Studies that recruited in the hospital demonstrated a significant reduction in mortality (relative risk 0.87, 95% confidence interval [CI] [0.76, 0.98]), HF readmissions (0.70, 95% CI [0.54, 0.89]), and all-cause readmissions (0.72, 95% CI [0.60, 0.87]). However, the difference in effect size between recruitment setting and involvement of primary care was not significant in a meta-regression analysis. Multidisciplinary HF DMPs that recruit in the community have no significant effect on mortality or hospital readmissions, unlike DMPs that recruit in the hospital, although the difference in effect size was not significant in a meta-regression analysis. Only six multidisciplinary studies involved primary care professionals. Given demographic evolutions and the importance of integrated home-based care for patients with HF, future multidisciplinary HF DMPs should consider integrating primary care professionals and evaluating the effectiveness of this model.
Keywords: care setting; community care; disease management; heart failure; multidisciplinary; primary care; transitional care.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures





References
-
- Dunlay SM, Roger VL, Redfield MM. Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol 2017; 14: 591–602. - PubMed
-
- Riegel B, LePetri R. Heart failure disease management models. In Moser D., Riegel B., eds. Improving Outcome in Heart Failure: An Interdisciplinary Approach. Maryland: Aspen; 2001: 267–281.
-
- Sochalski J, Jaarsma T, Krumholz HM, Laramee A, McMurray JJV, Naylor MD, Rich MW, Riegel B, Stewart S. What works in chronic care management: the case of heart failure. Health Aff 2009; 28: 179–189. - PubMed
-
- van Spall HGC, Rahman T, Mytton O, Ramasundarahettige C, Ibrahim Q, Kabali C, Coppens M, Brian Haynes R, Connolly S. Comparative effectiveness of transitional care services in patients discharged from the hospital with heart failure: a systematic review and network meta‐analysis. Eur J Heart Fail 2017; 19: 1427–1443. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
