

Antigen-Specific T-Cell Activation Distinguishes between Recent and Remote Tuberculosis Infection
- PMID: 33406011
- PMCID: PMC8483229
- DOI: 10.1164/rccm.202007-2686OC
Antigen-Specific T-Cell Activation Distinguishes between Recent and Remote Tuberculosis Infection
Abstract
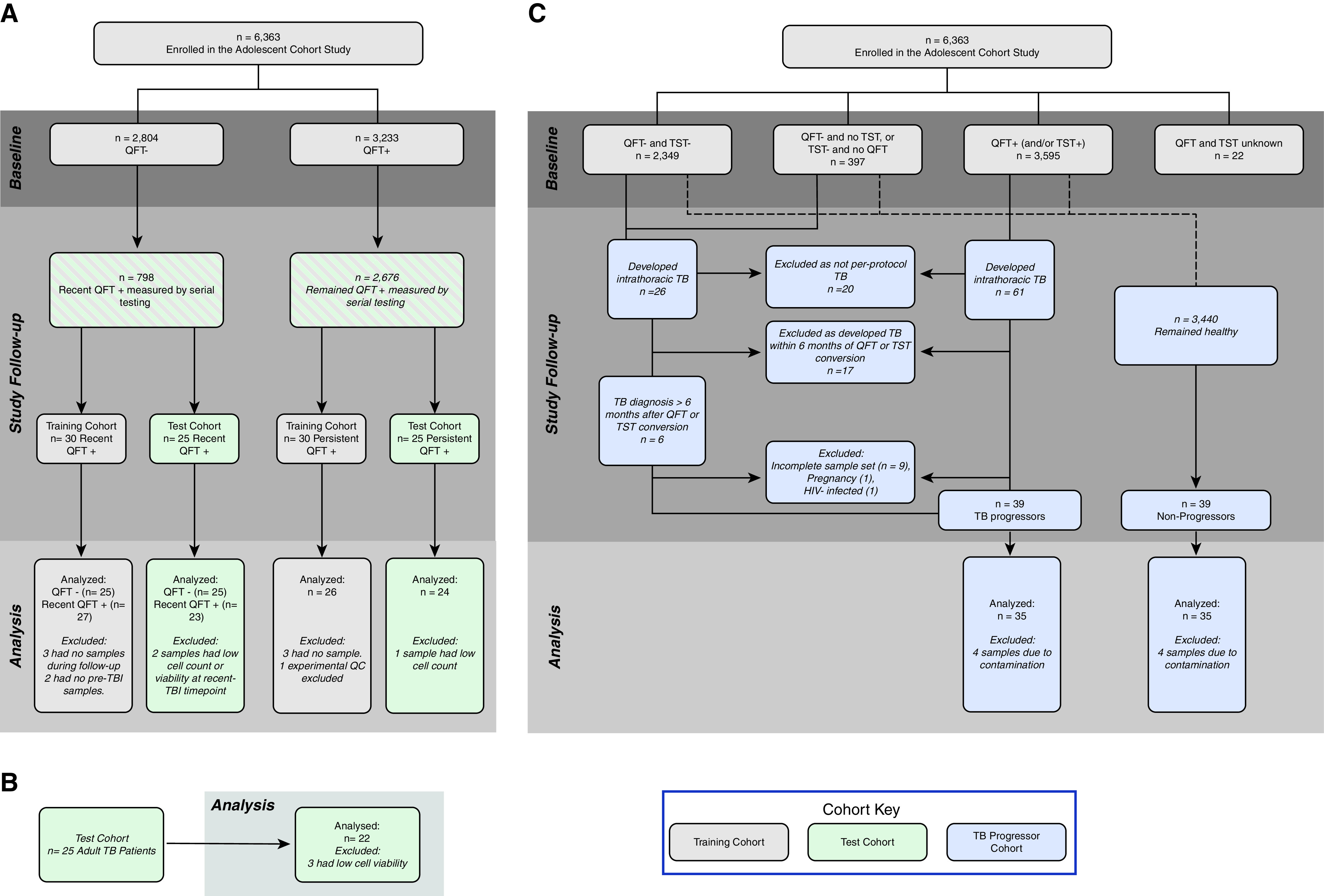
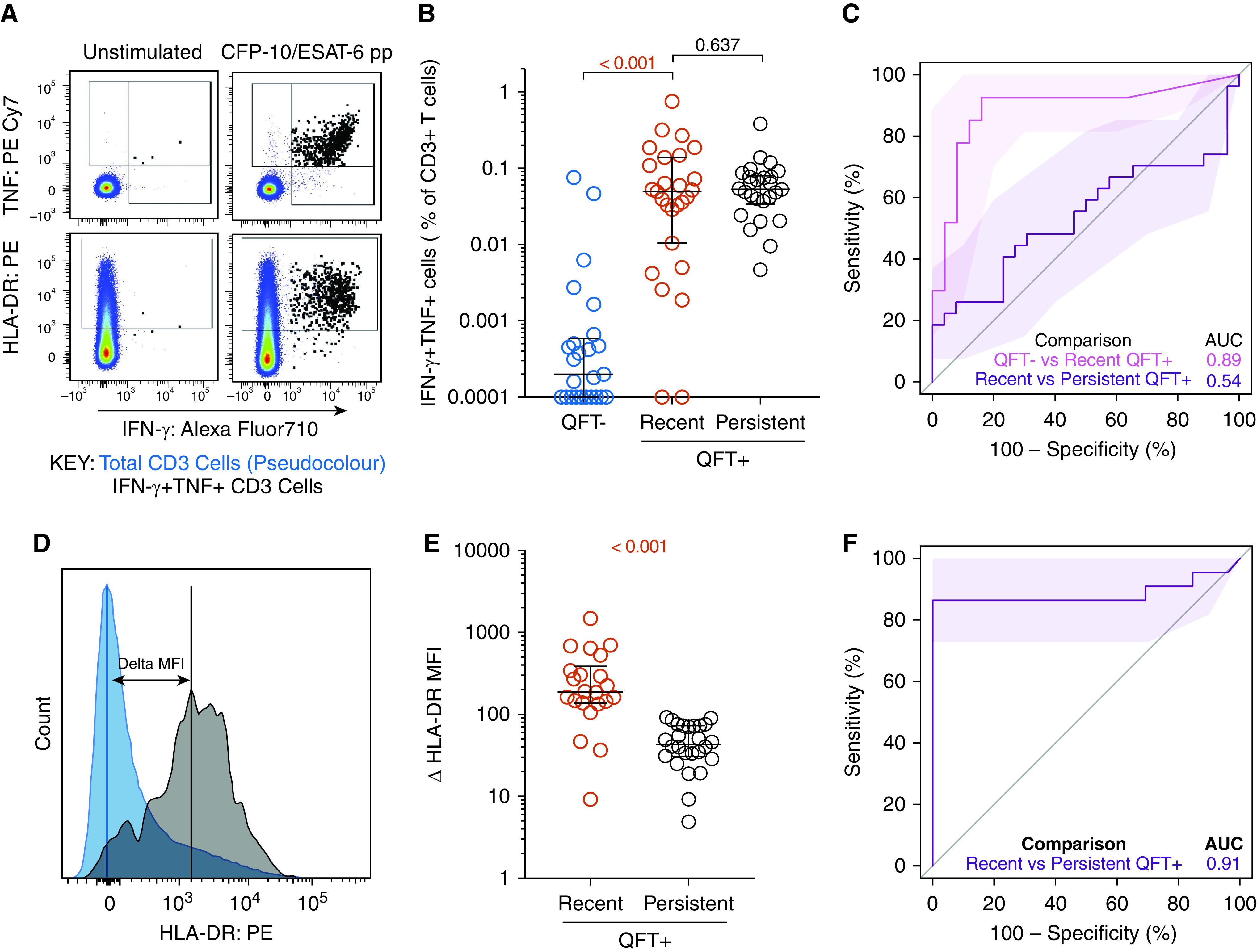
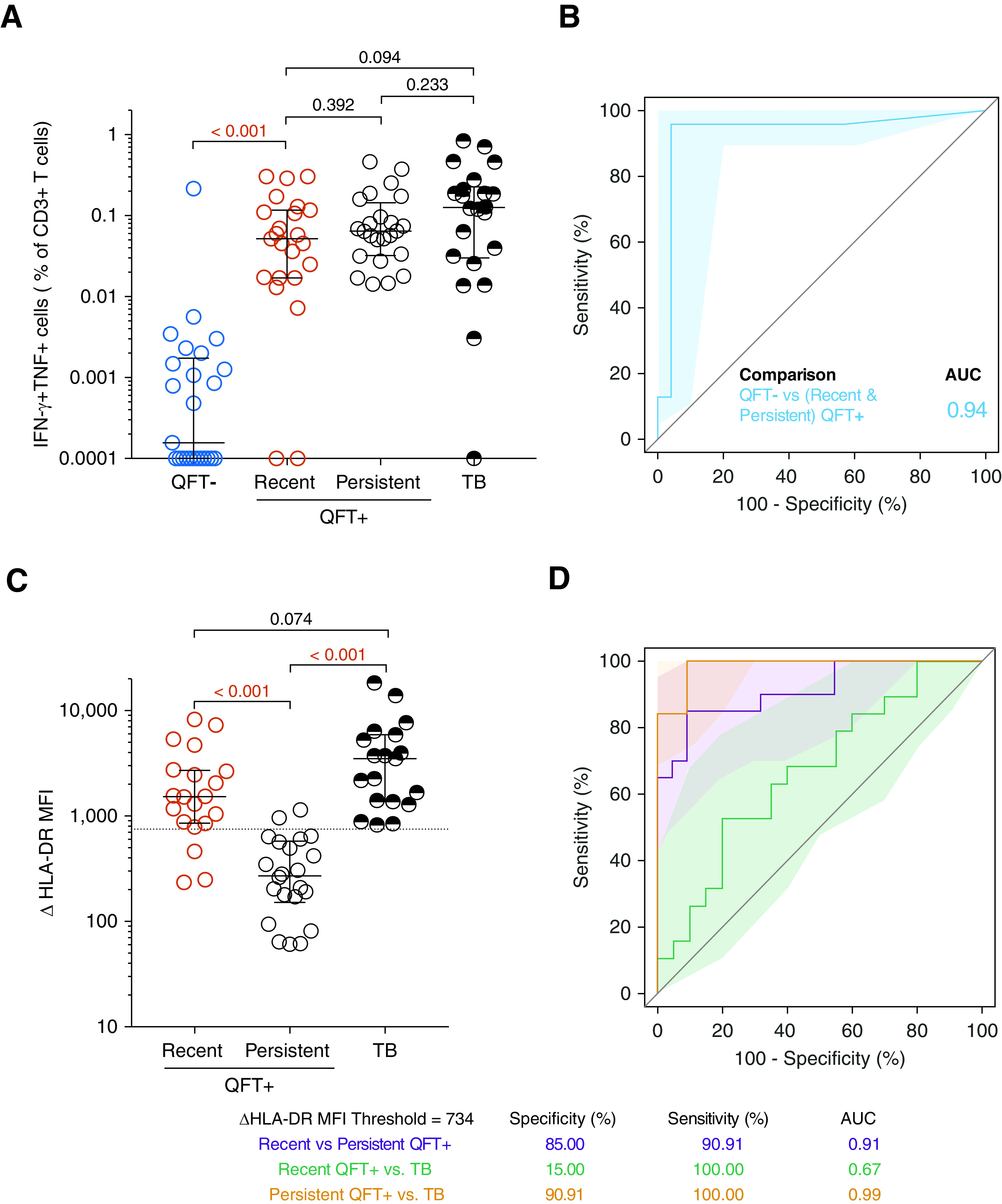
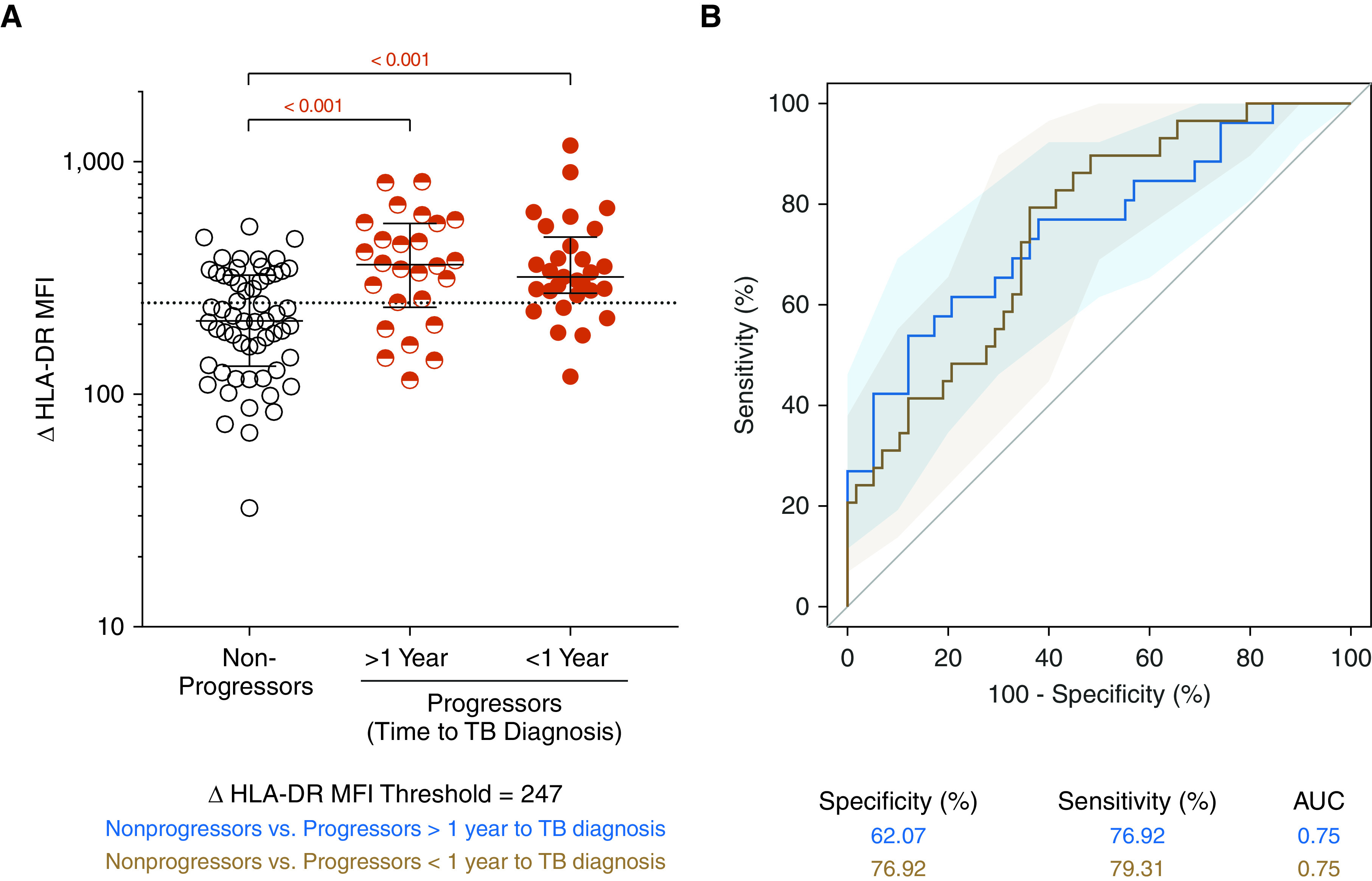
Rationale: Current diagnostic tests fail to identify individuals at higher risk of progression to tuberculosis disease, such as those with recent Mycobacterium tuberculosis infection, who should be prioritized for targeted preventive treatment. Objectives: To define a blood-based biomarker, measured with a simple flow cytometry assay, that can stratify different stages of tuberculosis infection to infer risk of disease. Methods: South African adolescents were serially tested with QuantiFERON-TB Gold to define recent (QuantiFERON-TB conversion <6 mo) and persistent (QuantiFERON-TB+ for >1 yr) infection. We defined the ΔHLA-DR median fluorescence intensity biomarker as the difference in HLA-DR expression between IFN-γ+ TNF+Mycobacterium tuberculosis-specific T cells and total CD3+ T cells. Biomarker performance was assessed by blinded prediction in untouched test cohorts with recent versus persistent infection or tuberculosis disease and by unblinded analysis of asymptomatic adolescents with tuberculosis infection who remained healthy (nonprogressors) or who progressed to microbiologically confirmed disease (progressors). Measurements and Main Results: In the test cohorts, frequencies of Mycobacterium tuberculosis-specific T cells differentiated between QuantiFERON-TB- (n = 25) and QuantiFERON-TB+ (n = 47) individuals (area under the receiver operating characteristic curve, 0.94; 95% confidence interval, 0.87-1.00). ΔHLA-DR significantly discriminated between recent (n = 20) and persistent (n = 22) QuantiFERON-TB+ (0.91; 0.83-1.00); persistent QuantiFERON-TB+ and newly diagnosed tuberculosis (n = 19; 0.99; 0.96-1.00); and tuberculosis progressors (n = 22) and nonprogressors (n = 34; 0.75; 0.63-0.87). However, ΔHLA-DR median fluorescent intensity could not discriminate between recent QuantiFERON-TB+ and tuberculosis (0.67; 0.50-0.84). Conclusions: The ΔHLA-DR biomarker can identify individuals with recent QuantiFERON-TB conversion and those with disease progression, allowing targeted provision of preventive treatment to those at highest risk of tuberculosis. Further validation studies of this novel immune biomarker in various settings and populations at risk are warranted.
Keywords: QuantiFERON-TB Gold; biomarker; recent tuberculosis infection; tuberculosis infection; tuberculosis risk.
Figures
Comment in
-
New Diagnostics to Infer Risk in Tuberculosis: Is the Term "Latent Tuberculosis Infection" Obsolete?Am J Respir Crit Care Med. 2021 Jun 15;203(12):1460-1461. doi: 10.1164/rccm.202101-0131ED. Am J Respir Crit Care Med. 2021. PMID: 33596391 Free PMC article. No abstract available.
References
-
- World Health Organization 2020https://www.who.int/tb/publications/global_report/en/.
-
- World Health Organization 2020https://www.who.int/publications-detail/who-consolidated-guidelines-on-t....
-
- Erkens CGM, Slump E, Verhagen M, Schimmel H, Cobelens F, van den Hof S. Risk of developing tuberculosis disease among persons diagnosed with latent tuberculosis infection in the Netherlands. Eur Respir J. 2016;48:1420–1428. - PubMed
-
- Reichler MR, Khan A, Sterling TR, Zhao H, Chen B, Yuan Y, et al. Tuberculosis Epidemiologic Studies Consortium Task Order 2 Team. Risk factors for tuberculosis and effect of preventive therapy among close contacts of persons with infectious tuberculosis. Clin Infect Dis. 2020;70:1562–1572. - PMC - PubMed
-
- Cohen A, Mathiasen VD, Schön T, Wejse C. The global prevalence of latent tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2019;54:1900655. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
