

Covert cases of Severe Acute Respiratory Syndrome Coronavirus 2: An obscure but present danger in regions endemic for Dengue and Chikungunya viruses
- PMID: 33406122
- PMCID: PMC7787539
- DOI: 10.1371/journal.pone.0244937
Covert cases of Severe Acute Respiratory Syndrome Coronavirus 2: An obscure but present danger in regions endemic for Dengue and Chikungunya viruses
Abstract
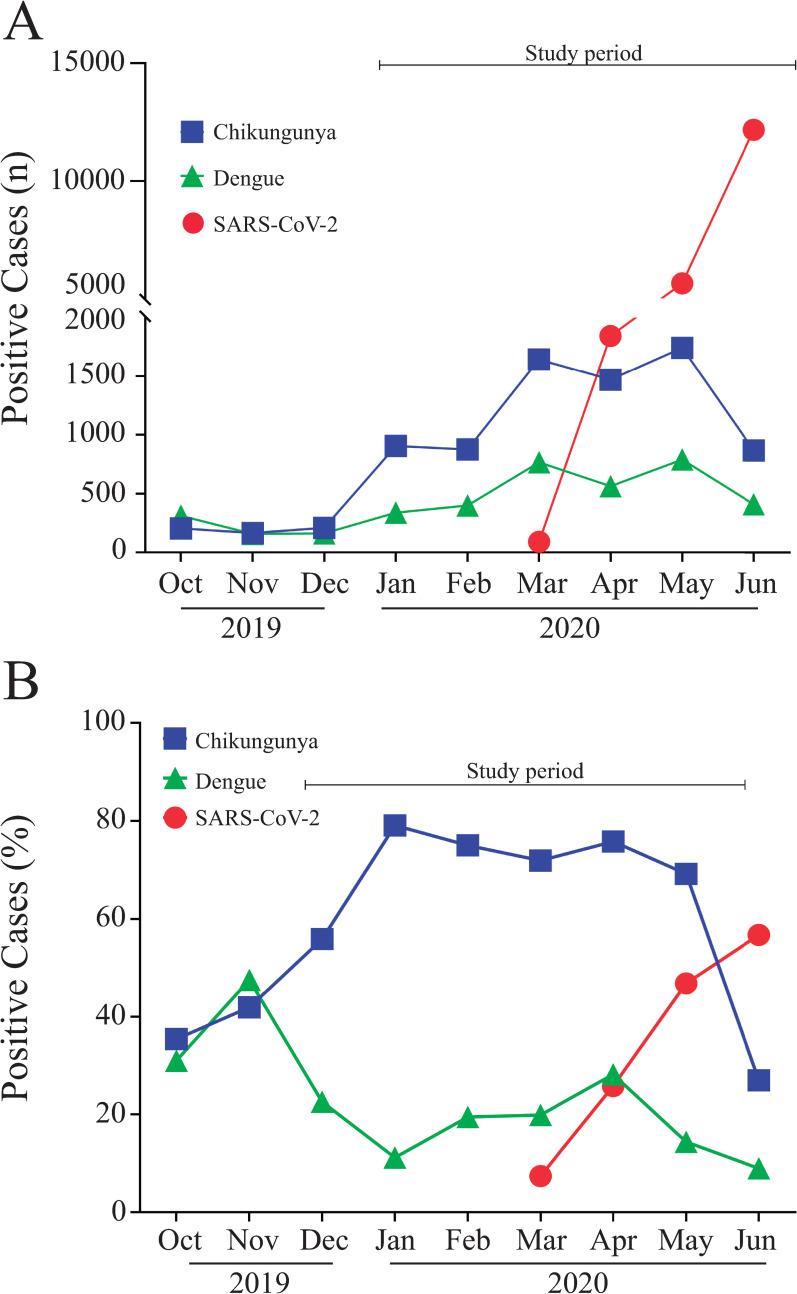
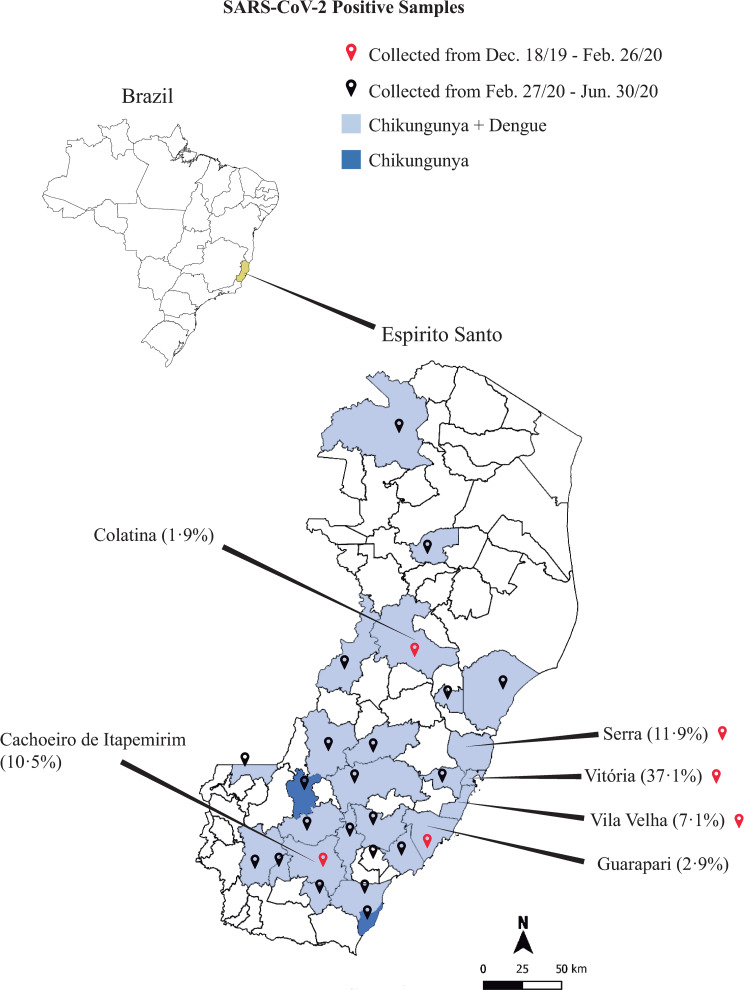
Background: The impact of SARS-CoV-2 in regions endemic for both Dengue and Chikungunya is still not fully understood. Considering that symptoms/clinical features displayed during Dengue, Chikungunya and SARS-CoV-2 acute infections are similar, undiagnosed cases of SARS-CoV-2 in co-endemic areas may be more prevalent than expected. This study was conducted to assess the prevalence of covert cases of SARS-CoV-2 among samples from patients with clinical symptoms compatible with either Dengue or Chikungunya viral infection in the state of Espírito Santo, Brazil.
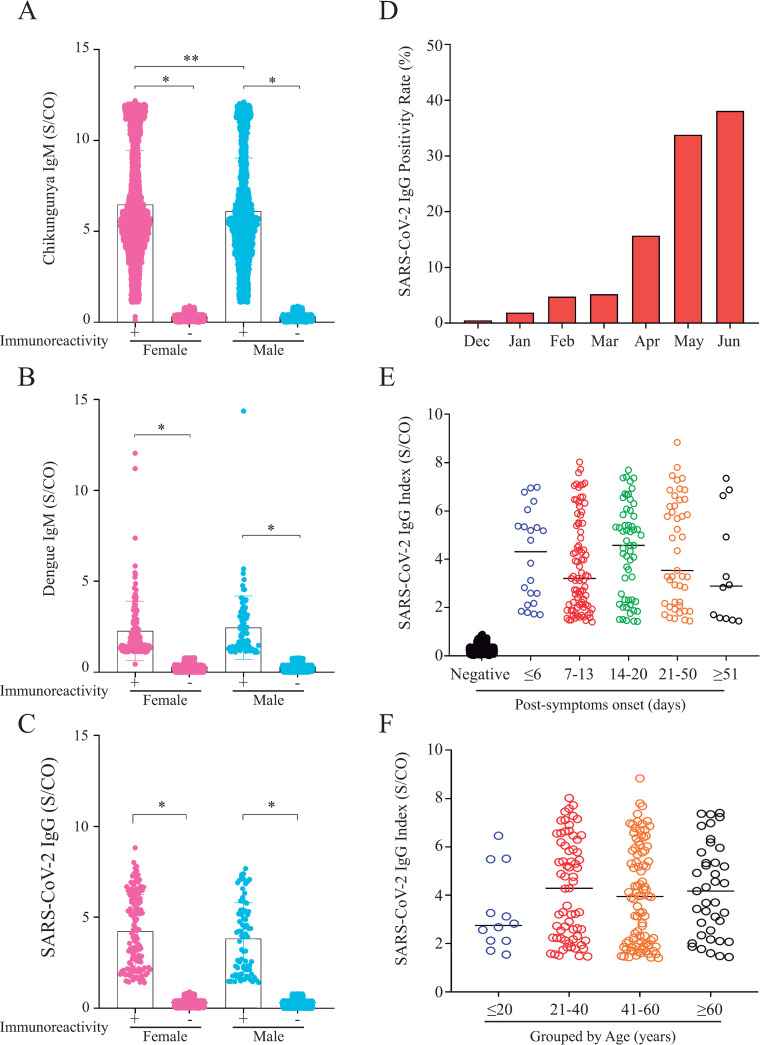
Methods: Presence of immunoglobulin G (IgG) antibody specific to SARS-CoV-2 nucleoprotein was detected using a chemiluminescent microparticle immunoassay in samples from 7,370 patients, without previous history of COVID-19 diagnosis, suspected of having either Dengue (n = 1,700) or Chikungunya (n = 7,349) from December 1st, 2019 to June 30th, 2020.
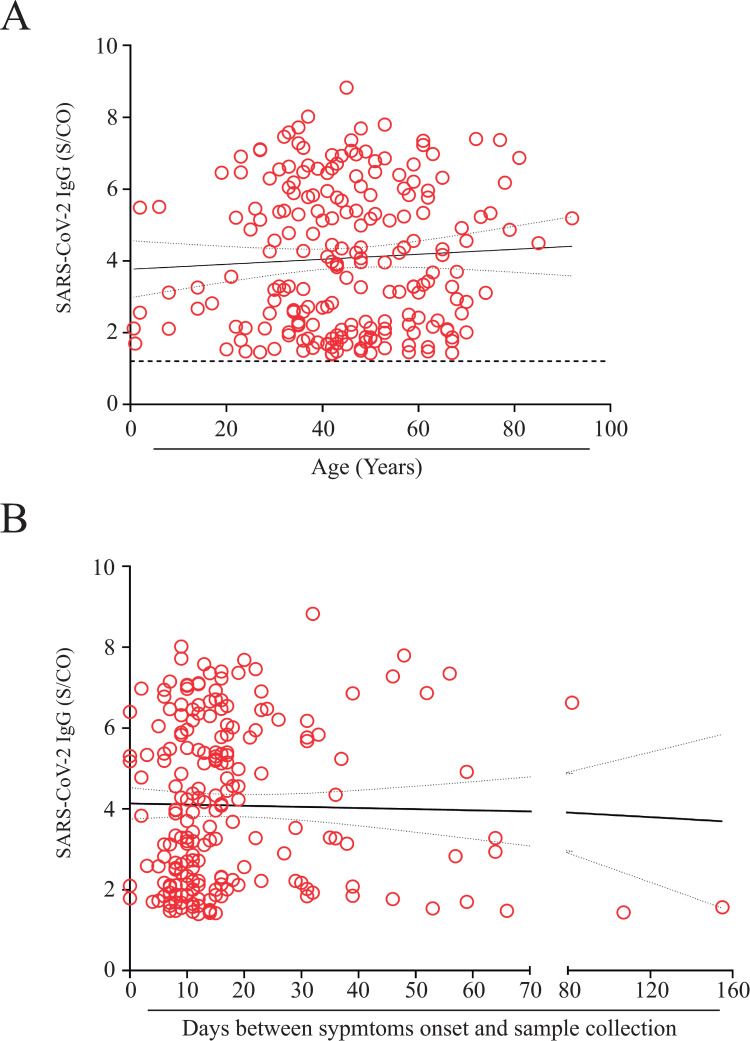
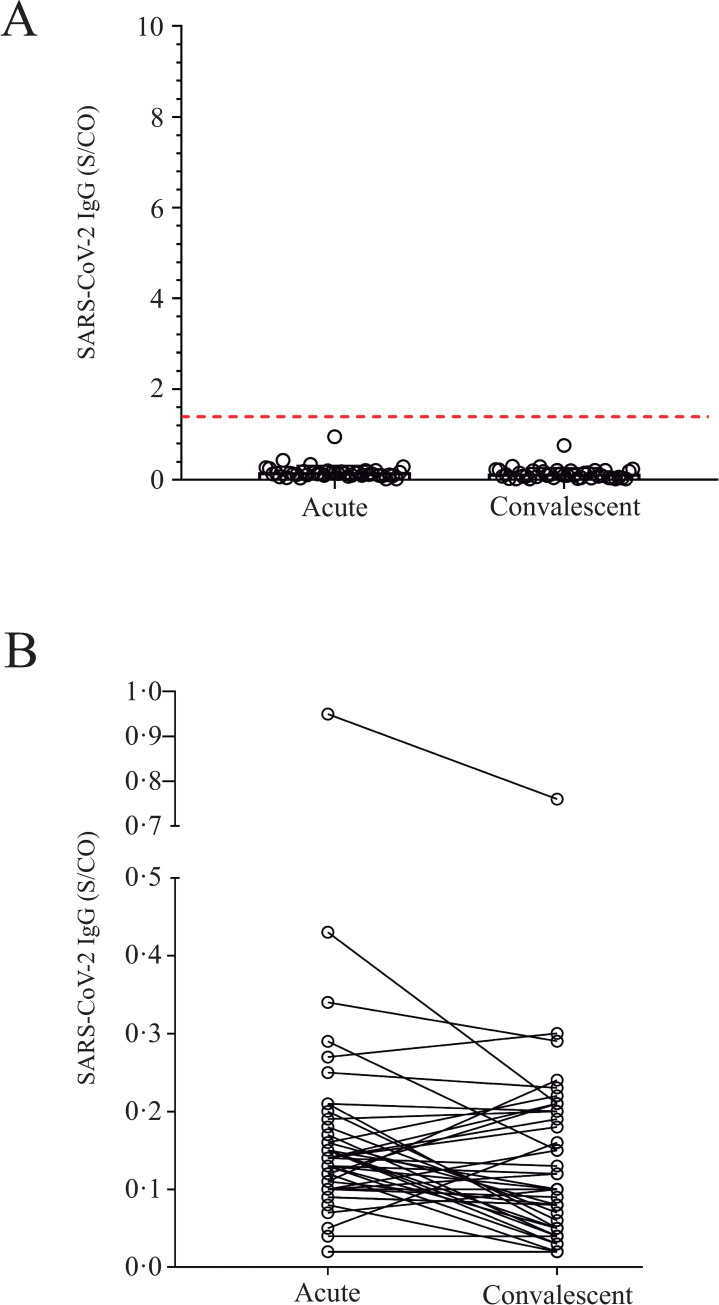
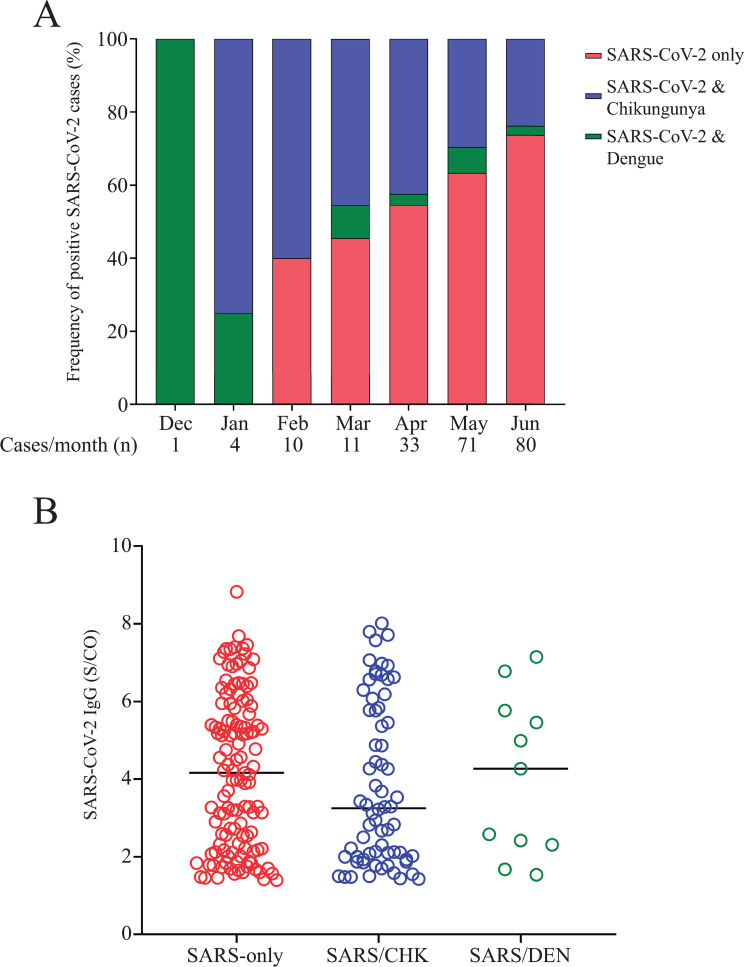
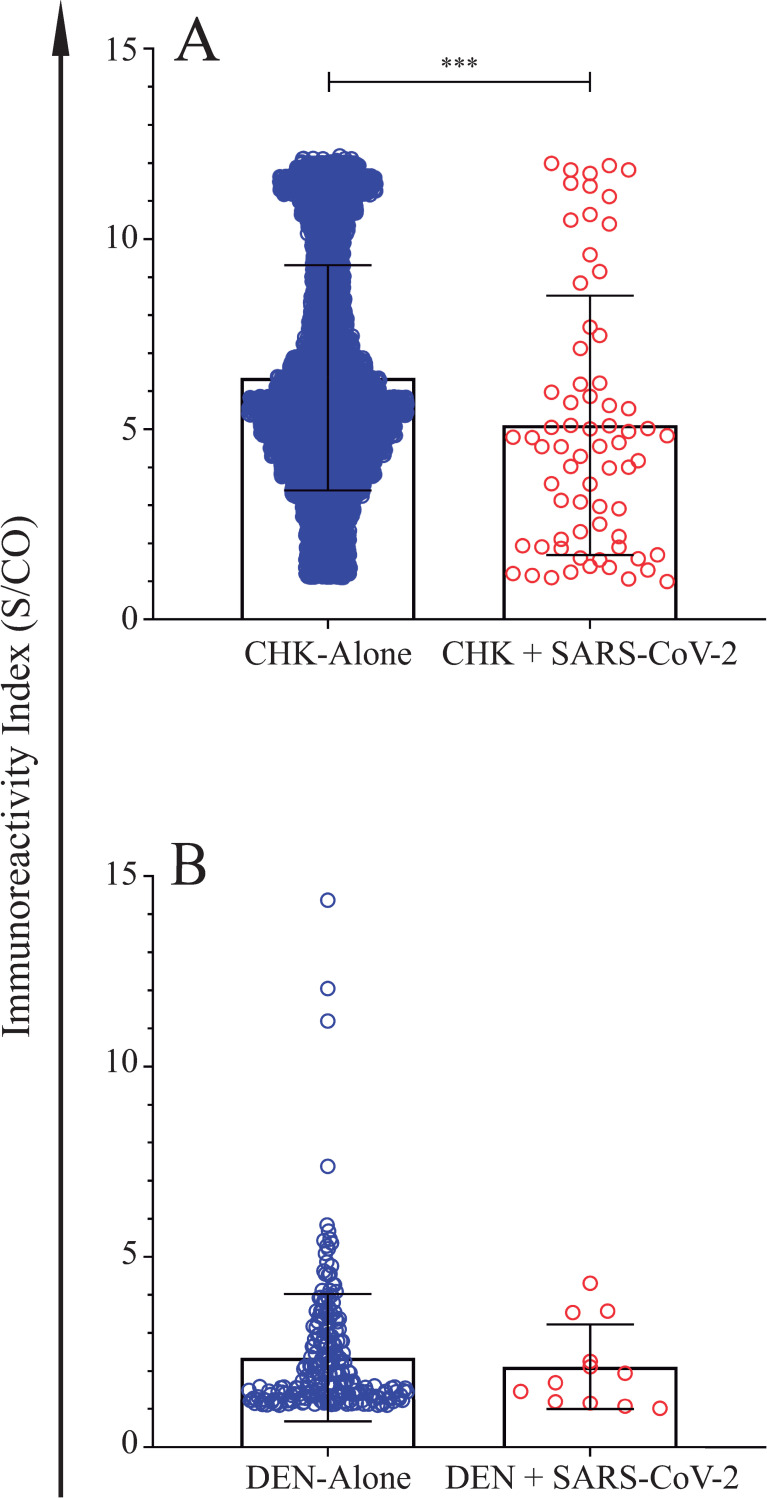
Findings: Covert cases of SARS-CoV-2 were detected in 210 (2.85%) out of the 7,370 serum samples tested. The earliest undiagnosed missed case of COVID-19 dated back to a sample collected on December 18, 2019, also positive for Dengue Virus. Cross-reactivity with either Dengue virus or other common coronaviruses were not observed.
Interpretation: Our findings demonstrate that concomitant Dengue or Chikungunya outbreaks may difficult the diagnosis of SARS-CoV-2 infections. To our knowledge, this is the first study to demonstrate, with a robust sample size (n = 7,370) and using highly specific and sensitive chemiluminescent microparticle immunoassay method, that covert SARS-CoV-2 infections are more frequent than previously expected in Dengue and Chikungunya hyperendemic regions. Moreover, our results suggest that SAR-CoV-2 cases were occurring prior to February, 2020, and that these undiagnosed missed cases may have contributed to the fast expansion of SARS-CoV-2 outbreak in Brazil. Data presented here demonstrate that in arboviral endemic regions, SARS-CoV-2 infection must be always considered, regardless of the existence of a previous positive diagnosis for Dengue or Chikungunya.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Petrosillo N, Viceconte G, Ergonul O, Ippolito G, Petersen E. COVID-19, SARS and MERS: are they closely related? Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2020;26(6):729–34. Epub 2020/04/03. 10.1016/j.cmi.2020.03.026 - DOI - PMC - PubMed
-
- W.H.O. Coronavirus disease (COVID-2019) situation reports 2020: World Health Organization; 2020 [cited 2020 01/09/2020]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
